Mississippi Today
Mississippi jailed more than 800 people awaiting psychiatric treatment in a year. Just one jail meets state standards.

This article was produced for ProPublica’s Local Reporting Network in partnership with Mississippi Today. Sign up for Dispatches to get stories like this one as soon as they are published.
In Mississippi, many people awaiting court-ordered treatment for mental illness or substance abuse are jailed, even though they haven’t been charged with a crime. Read our full series here.
Fourteen years ago, Mississippi legislators passed a law requiring county jails to be certified by the state if they held people awaiting court-ordered psychiatric treatment.
Today, just one jail in the state is certified.
And yet, from July 2022 to June 2023, more than 800 people awaiting treatment were jailed throughout the state, almost all in uncertified facilities, according to state data.
Mississippi Today and ProPublica have been reporting on county officials’ practice of jailing people with mental illness, most of whom haven’t been charged with a crime, as they await treatment under the state’s civil commitment law. After the news organizations started asking about the 2009 law earlier this year, the state attorney general’s office concluded that it is a “mandatory requirement” that the Mississippi Department of Mental Health certify the facilities where people are held after judges have ordered them into treatment.
The Department of Mental Health, which oversees the state’s behavioral health system and has no other responsibility for jails, responded by sending letters to county officials across the state encouraging them to stop holding people in uncertified jails. But the law provides no funding to help counties comply and no penalties if they don’t.
Under state law, counties are responsible for housing people going through the commitment process until they are admitted to a state hospital. Counties are allowed to put them in jail before their court hearings if there’s “no reasonable alternative.”
The last time the Department of Mental Health tried to ensure those jails met state standards, more than a decade ago, it had little success. After the law passed, the agency got to work to inform counties about the new rules. Some didn’t respond. Others expressed interest but didn’t follow through. By 2013, just two jails had been certified. (One of them no longer is.) After that, the effort apparently petered out, according to a review of state documents.
To be certified, a jail must offer on-call crisis care by a physician or psychiatric nurse practitioner and must have a supply of medications. Staff must be trained in crisis intervention and suicide prevention. People detained during the commitment process must be housed separately from people charged with crimes, in rooms free of fixtures or structures that could be used for self-harm, according to Department of Mental Health standards that took effect in 2011.
“If they’re going to be held in jail, they have to receive some kind of treatment in a semi-safe environment,” a department attorney told The Clarion-Ledger at the time.
Until recently, many county officials weren’t even aware of those requirements, according to interviews across the state — even though they were routinely jailing people solely because they might need mental health treatment. Mississippi appears to be the only state in the country where people awaiting treatment are commonly jailed without charges for days or weeks at a time.
Mississippi jails are subject to no statewide health and safety standards. Many jails treat people going through the civil commitment process virtually the same as those who have been charged with crimes, Mississippi Today and ProPublica found. They’re shackled and given jail uniforms. They’re often held in the same cells as criminal defendants. They receive minimal medical care. Some said they couldn’t access prescribed psychiatric medications. Since 1987, at least 18 people going through the commitment process for mental illness and substance abuse have died after being jailed, most of them by suicide.

Some local officials say getting certified could be expensive. Sheriffs worry it could codify their role as their county’s de facto mental health care provider.
“It looks like the state wants the sheriff to be the chief mental health officer,” said Will Allen, attorney for the Mississippi Sheriffs’ Association. “This is coming down to the state stuffing the cost of this down to the counties, and frankly I just think that’s wrong.”
‘Are you going to shut the jail down? No.’
The genesis of the 2009 law was a conversation state Sen. Joey Fillingane had with his girlfriend at the time, a social worker who worked with troubled youth. She told him that Mississippians going through the commitment process in some counties were locked in jail cells like criminals, while in other counties they were held in hospitals like patients, according to a 2011 news story in The Clarion-Ledger.
Fillingane’s bill addressed that. “Shouldn’t there be some kind of minimum standard where you’re holding people who haven’t committed a crime?” the Republican from Sumrall, near Hattiesburg, said in that story about his legislation.
His bill passed with little fanfare. It made it “illegal for individuals committed to a DMH behavioral health program to be held in jail unless it had been certified” as a holding facility, an agency staffer wrote in a timeline of the law’s implementation obtained by Mississippi Today and ProPublica.
The board overseeing the Department of Mental Health set detailed standards for those facilities. Department staff surveyed counties to see whether they could meet them.
Ed LeGrand was head of the department when the law passed. He said he viewed it as a progressive effort that could spur counties to stop holding mentally ill people in jail. And even if that didn’t happen, the law would improve jail conditions — at least somewhat.
“I didn’t think that everybody would be able to meet those standards. I thought they would give it a try,” he said in a recent interview. “A lot of them did, but some of them didn’t.”
Department staff met with county officials and toured jails to offer assistance. Those visits, which records show mostly took place in 2011 and 2012, were the first time the Department of Mental Health had tried to get a comprehensive look at the local facilities where Mississippians awaited psychiatric treatment in state hospitals, LeGrand said.
Many jails were poorly equipped to care for these people, according to notes by agency staff.
“Toured the current jail (scary),” reads a status update written after staff visited Tishomingo County, in the northeast corner of the state, shortly before the county opened a new jail. In Jones County in south Mississippi, where the jail had 180 inmates and only four staff: “The holding cells are not safe for violent behavior. Too much cement.”
Jones County Sheriff Joe Berlin said the cells have not changed since then, though now detainees are monitored with cameras.
In early 2011, LeGrand told county officials who hadn’t already begun the certification process that they had six months to find a certified provider to house people awaiting treatment.
Sheriffs were frustrated. Some objected to being told they had to upgrade their jails and train guards so they could care for mentally ill people they didn’t think they should be responsible for in the first place.
“What do they expect of me?” one sheriff was quoted as saying in the 2011 news story. “What they need to do is turn around and certify some places that are under Mental Health’s control so they can be responsible for it, not me.”

Some county officials concluded there was little the state could do if they didn’t comply. Mike Harlin, the jail administrator in Lamar County, discussed the standards with a Department of Mental Health staffer in 2012, according to an agency memo. In an interview this year, Harlin said he remembered thinking, “What are you going to do? Are you going to shut the jail down? No.”
By June 2013, jails in just two of the state’s 82 counties had been certified, according to the department’s tally. (A hospital was certified in another county, and a different type of facility was certified in a fourth.)
Six counties said they couldn’t meet the standards. Another 23 had received guidance from the department on how to meet them. Thirty, including a few of the counties that had received advice, eventually said they didn’t jail people, some because they had contracts with providers. Twenty-one never responded.
Mississippi Today and ProPublica requested all Department of Mental Health records since 2010 related to enforcement of the certification law and correspondence with counties. Documents through 2013 included standards, correspondence, memos describing visits to county facilities and a log summarizing contact with each county. After that, the records released show no statewide outreach.
The final entry in the department’s timeline of the law’s implementation reads: “June 2013 was the last attempt to update the information about DMH Designated Mental Health Holding Facilities due to lack of additional responses from the counties.” That timeline is undated, but a department spokesperson said data in the file shows that it was created in January 2015 by a staffer who held positions in the certification and behavioral health divisions.
LeGrand, who served until 2014, said he doesn’t recall any decision to stop contacting counties about the law.
Katie Storr, the current chief of staff at the Department of Mental Health, told Mississippi Today and ProPublica it’s possible staff did communicate with counties beyond what the records indicate. “After more than a decade, a lack of correspondence, email, or other documentation is not indicative that communication and follow-ups did not take place,” she wrote in an email. However, she said the department had no additional records that would show this.
During this time, Storr wrote, the department was focused on trying to get counties to hold people going through the commitment process in short-term crisis stabilization units rather than jail.
Department can’t ‘boss counties around’
The recent effort to implement the certification law stems from inquiries by Mississippi Today and ProPublica.
In January, the news organizations asked the head of the Department of Mental Health, Wendy Bailey, if the department certifies jails where people are held as they await admission to a state hospital. Bailey, who handled communications for the department when the certification law passed, initially said it didn’t apply to jails. In March, after reviewing documents showing prior efforts to certify jails, she said she didn’t believe the law was intended to apply to them.
After our inquiries, Bailey sought an opinion from the attorney general. (Such opinions are not binding, but officials who request and abide by them are protected from liability.)
Around the same time, the Department of Mental Health contacted the four facilities it had previously certified to schedule inspections. The department’s standards say such inspections will happen annually, but this was the first year in which staff had sought to visit all of them since 2017. (Storr said the inspection effort was planned before inquiries by Mississippi Today and ProPublica.)
In March, staffers inspecting the Chickasaw County jail in rural northeastern Mississippi found serious violations. Inmates and people awaiting mental health treatment were housed together in the same cells, where beds were anchored with long bolts that “could be used by a person to harm themselves,” the reviewers recorded.
The department suspended the jail’s certification in August, but reinstated it after the county submitted a compliance plan that included shortening the bolts and providing mental health training for staff.
Lafayette County told the state it didn’t want its jail to be certified anymore. The certification for a holding facility in Warren County, home to Vicksburg, was suspended. A hospital in Alcorn County in northeast Mississippi maintained its certification.

In August, the attorney general’s office confirmed that the department must “ensure that each county holding facility, including but not limited to county jails,” meets its standards. If they don’t, an assistant attorney general wrote, the law allows the department to require counties to contract with a county that does have a certified facility.
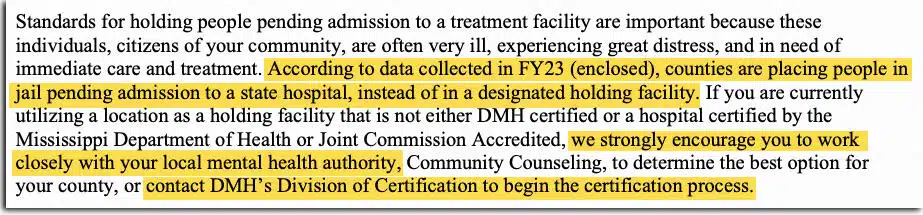
When Bailey informed county officials about the opinion in her October letter, she instructed that if a county holds someone in an uncertified facility, including a jail, officials should contact the department to seek certification or work with local community mental health centers. These are publicly funded, independent providers set up to ensure that poor, uninsured people can access mental health care.
Several counties, including Lamar, have taken up the matter in public meetings or have contacted the department to begin the certification process.
Storr told Mississippi Today and ProPublica that the department asked counties to initiate the certification process because the law says it’s up to counties to determine which facility they use.
But the Department of Mental Health already knows which counties have held people in uncertified jails. Starting in July 2021, in response to a federal lawsuit over the state’s mental health system, department staff have tracked how many people come to state hospitals directly from jails for psychiatric treatment.
The tally for the year ending in June breaks down all 71 jails, only one of which is certified, where a total of 812 people who had been civilly committed were held before being admitted to a state hospital. (The tally doesn’t include anyone who was jailed and released without being admitted to a state hospital.)
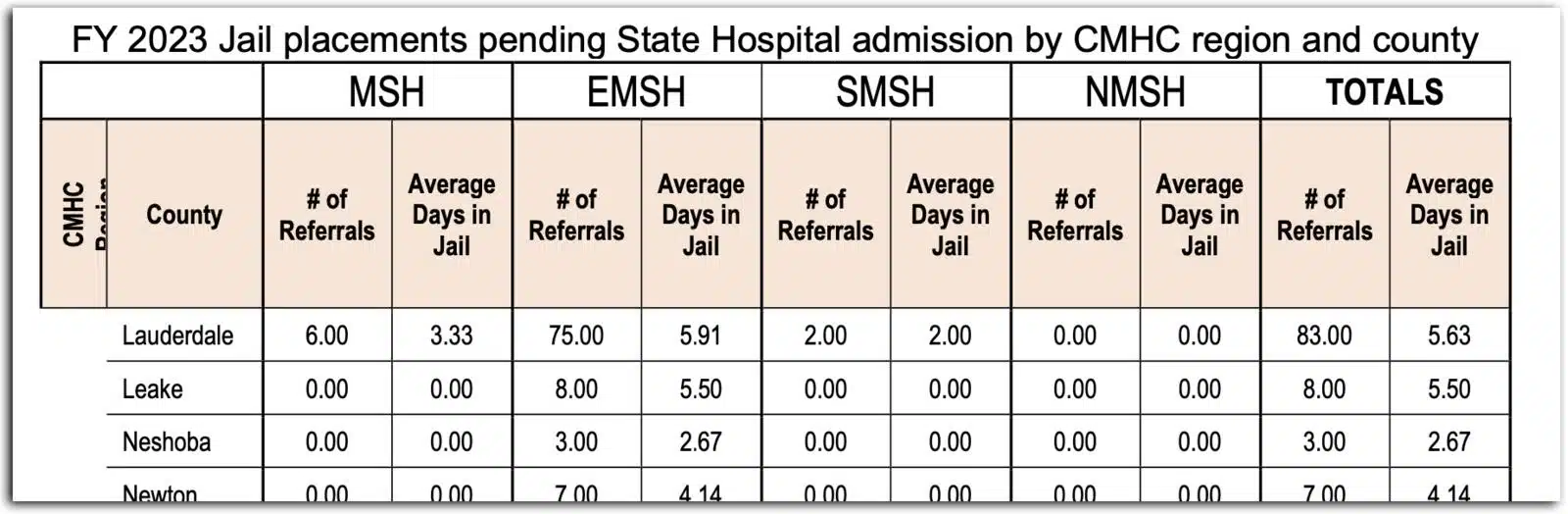
In Lauderdale County, on the Alabama line: 83. Across the state in DeSoto County: 76. A couple hundred miles down the Mississippi River in Adams County: 33.
Storr and Bailey have emphasized that they have limited authority over counties and no way to force them to do anything. The department’s only means of enforcement, Storr wrote, is to put a jail on probation, then revoke certification — if the jail in question even was certified in the first place — and require the county to contract with another provider.
LeGrand said a law without teeth is effectively optional. “The department’s not really in a good position to boss counties around,” he said.
James Tucker, an attorney and the director of the Alabama Disabilities Advocacy Program, which has sued that state over its civil commitment process, said the agency has a responsibility to make sure counties are treating people properly. “You don’t discharge that duty by sitting on your hands and waiting for every local sheriff to report in,” he said.
Bailey’s department encourages counties to connect families with outpatient services in order to avoid the commitment process. If someone does need to be committed, the department said, counties should hold people in crisis stabilization units operated by community mental health centers.
“I do not believe jails are an appropriate location to hold someone who is not charged with a crime and is awaiting admission to a treatment bed,” Bailey told Mississippi Today and ProPublica in an email. “The person should be in a safe location, receiving treatment.”

But there are only 180 crisis beds in the state, and crisis stabilization units frequently turn people away because they are full, can’t provide the needed care, or deem a patient too violent. Storr said the agency is working to reduce denials and plans to use one-time federal pandemic funding to expand capacity.
Allen, the sheriffs’ association attorney, said the state will need more crisis beds if officials want to keep people out of jail as they await mental health care. He said he’s been meeting with sheriffs and county officials since the guidance was issued.
“This has catalyzed the county governments and law enforcement to do something,” he said. Sheriffs agree on the need for “certified centers, just not in the county jail.”
Mollie Simon of ProPublica contributed research to this story.
This article first appeared on Mississippi Today and is republished here under a Creative Commons license.

Did you miss our previous article…
https://www.biloxinewsevents.com/?p=304973











President Donald Trump on Tuesday nominated Baxter Kruger to become Mississippi’s new U.S. attorney in the Southern District and Scott Leary to become U.S. attorney for the Northern District.
The two nominations will head to the U.S. Senate for consideration. If confirmed, the two will oversee federal criminal prosecutions and investigations in the state.
Kruger graduated from the Mississippi College School of Law in 2015 and was previously an assistant U.S. attorney for the Southern District. He is currently the director of the Mississippi Office of Homeland Security.
Sean Tindell, the Mississippi Department of Public Safety commissioner, oversees the state’s Homeland Security Office. He congratulated Kruger on social media and praised his leadership at the agency.
“Thank you for your outstanding leadership at the Mississippi Office of Homeland Security and for your dedicated service to our state,” Tindell wrote. “Your hard work and commitment have not gone unnoticed and this nomination is a testament to that!”
Leary graduated from the University of Mississippi School of Law, and he has been a federal prosecutor for most of his career.
He worked for the U.S. Attorney’s Office in the Western District of Tennessee in Memphis from 2002 to 2008. Afterward, he worked at the U.S. Attorney’s Office for the Northern District of Mississippi in Oxford, where he is currently employed.
Leary told Mississippi Today that he is honored to be nominated for the position, and he looks forward to the Senate confirmation process.
This article first appeared on Mississippi Today and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
The post Trump nominates Baxter Kruger, Scott Leary for Mississippi U.S. attorney posts appeared first on mississippitoday.org

Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Centrist
This article presents a straightforward news report on President Donald Trump’s nominations of Baxter Kruger and Scott Leary for U.S. attorney positions in Mississippi. It focuses on factual details about their backgrounds, qualifications, and official responses without employing loaded language or framing that favors a particular ideological perspective. The tone is neutral, with quotes and descriptions that serve to inform rather than persuade. While it reports on a political appointment by a Republican president, the coverage remains balanced and refrains from editorializing, thus adhering to neutral, factual reporting.
After more than 10 months closed due to mold, asbestos and issues with the air conditioning system, Thalia Mara Hall has officially reopened.
Outgoing Mayor Chokwe A. Lumumba announced the reopening of Thalia Mara Hall during his final press conference held Monday on the arts venue’s steps.
“Today marks what we view as a full circle moment, rejoicing in the iconic space where community has come together for decades in the city of Jackson,” Lumumba said. “Thalia Mara has always been more than a venue. It has been a gathering place for people in the city of Jackson. From its first class ballet performances to gospel concerts, Thalia Mara Hall has been the backdrop for our city’s rich cultural history.”
Thalia Mara Hall closed last August after mold was found in parts of the building. The issues compounded from there, with malfunctioning HVAC systems and asbestos remediation. On June 6, the Mississippi State Fire Marshal’s Office announced that Thalia Mara Hall had finally passed inspection.
“We’re not only excited to have overcome many of the challenges that led to it being shuttered for a period of time,” Lumumba said. “We are hopeful for the future of this auditorium, that it may be able to provide a more up-to-date experience for residents, inviting shows that people are able to see across the world, bringing them here to Jackson. So this is an investment in the future.”
In total, Emad Al-Turk, a city contracted engineer and owner of Al-Turk Planning, estimates that $5 million in city and state funds went into bringing Thalia Mara Hall up to code.
The venue still has work to be completed, including reinstalling the fire curtain. The beam in which the fire curtain will be anchored has asbestos in it, so it will have to be remediated. In addition, a second air-conditioning chiller needs to be installed to properly cool the building. Until it’s installed, which could take months, Thalia Mara Hall will be operating at a lower seating capacity of about 800.
“Primarily because of the heat,” Al-Turk said. “The air conditioning would not be sufficient to actually accommodate the 2,000 people at full capacity, but starting in the fall, that should not be a problem.”
Al-Turk said the calendar is open for the city to begin booking events, though none have been scheduled for July.
“We’re very proud,” he said. “This took a little bit longer than what we anticipated, but we had probably seven or eight different contractors we had to coordinate with and all of them did a superb job to get us where we are today.”
This article first appeared on Mississippi Today and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
The post Jackson’s performing arts venue Thalia Mara Hall is now open appeared first on mississippitoday.org
Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Centrist
The article presents a straightforward report on the reopening of Thalia Mara Hall in Jackson, focusing on facts and statements from city officials without promoting any ideological viewpoint. The tone is neutral and positive, emphasizing the community and cultural significance of the venue while detailing the challenges overcome during renovations. The coverage centers on public investment and future prospects, without partisan framing or editorializing. While quotes from Mayor Lumumba and a city engineer highlight optimism and civic pride, the article maintains balanced, factual reporting rather than advancing a political agenda.
Mississippi Today
‘Hurdles waiting in the shadows’: Lumumba reflects on challenges and triumphs on final day as Jackson mayor
On his last day as mayor of Jackson, Chokwe Antar Lumumba recounted accomplishments, praised his executive team and said he has no plans to seek office again.
He spoke during a press conference outside of the city’s Thalia Mara Hall, which was recently cleared for reopening after nearly a year of remediation. The briefing, meant to give media members a peek inside the downtown theater, marked one of Lumumba’s final forays as mayor.
Longtime state Sen. John Horhn — who defeated Lumumba in the Democratic primary runoff — will be inaugurated as mayor Tuesday, but Lumumba won’t be present. Not for any contentious reason, the 42-year-old mayor noted, but because he returns to his private law practice Tuesday.
“I’ve got to work now, y’all,” Lumumba said. “I’ve got a job.”
Thalia Mara Hall’s presumptive comeback was a fitting end for Lumumba, who pledged to make Jackson the most radical city in America but instead spent much of his eight years in office parrying one emergency after another. The auditorium was built in 1968 and closed nearly 11 months ago after workers found mold caused by a faulty HVAC system – on top of broken elevators, fire safety concerns and vandalism.
“This job is a fast-pitched sport,” Lumumba said. “There’s an abundance of challenges that have to be addressed, and it seems like the moment that you’ve gotten over one hurdle, there’s another one that is waiting in the shadows.”
Outside the theater Monday, Lumumba reflected on the high points of his leadership instead of the many crises — some seemingly self-inflicted — he faced as mayor.
He presided over the city during the coronavirus pandemic and the rise in crime it brought, but also the one-two punch of the 2021 and 2022 water crises, exacerbated by the city’s mismanagement of its water plants, and the 18-day pause in trash pickup spurred by Lumumba’s contentious negotiations with the city council in 2023.
Then in 2024, Lumumba was indicted alongside other city and county officials in a sweeping federal corruption probe targeting the proposed development of a hotel across from the city’s convention center, a project that has remained stalled in a 20-year saga of failed bids and political consternation.
Slated for trial next year, Lumumba has repeatedly maintained his innocence.
The city’s youngest mayor also brought some victories to Jackson, particularly in his first year in office. In 2017, he ended a furlough of city employees and worked with then-Gov. Phil Bryant to avoid a state takeover of Jackson Public Schools. In 2019, the city successfully sued German engineering firm Siemens and its local contractors for $89 million over botched work installing the city’s water-sewer billing infrastructure.
“I think that that was a pivotal moment to say that this city is going to hold people responsible for the work that they do,” Lumumba said.
Lumumba had more time than any other mayor to usher in the 1% sales tax, which residents approved in 2014 to fund infrastructure improvements.
“We paved 144 streets,” he said. “There are residents that still are waiting on their roads to be repaved. And you don’t really feel it until it’s your street that gets repaved, but that is a significant undertaking.”
And under his administration, crime has fallen dramatically recently, with homicides cut by a third and shootings cut in half in the last year.
Lumumba was first elected in 2017 after defeating Tony Yarber, a business-friendly mayor who faced his own scandals as mayor. A criminal justice attorney, Lumumba said he never planned to seek office until the stunning death of his father, Chokwe Lumumba Sr., eight months into his first term as mayor in 2014.
“I can say without reservation, and unequivocally, we remember where we started. We are in a much better position than we started,” Lumumba said.
Lumumba said he has sat down with Horhn in recent months, answered questions “as extensively as I could,” and promised to remain reachable to the new mayor.
This article first appeared on Mississippi Today and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
The post 'Hurdles waiting in the shadows': Lumumba reflects on challenges and triumphs on final day as Jackson mayor appeared first on mississippitoday.org
Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Center-Left
The article reports on outgoing Jackson Mayor Chokwe Antar Lumumba’s reflections without overt editorializing but subtly frames his tenure within progressive contexts, emphasizing his self-described goal to make Jackson “the most radical city in America.” The piece highlights his accomplishments alongside challenges, including public crises and a federal indictment, maintaining a factual tone yet noting contentious moments like labor disputes and governance issues. While it avoids partisan rhetoric, the focus on social justice efforts, infrastructure investment, and crime reduction, as well as positive framing of Lumumba’s achievements, aligns with a center-left perspective that values progressive governance and accountability.

Democrats blocked from inspecting Florida’s Everglades detention site

Why Mississippians Love Independence Day

How the AcA brought Kandinsky to kindergarten – The Current

House sends GOP’s ‘big, beautiful bill’ to Trump’s desk in major win for Republicans

Ole Miss chancellor Glenn Boyce elected to SEC Executive Committee

Michael Madsen of ‘Kill Bill’ and ‘Reservoir Dogs’ dies: reports

Building housing fireworks goes up in flames after electric box fire

What’s happening with the money Travis County approved for affordable child care?

Fireworks Safety Tips

Sean 'Diddy' Combs found guilty on 2 of 5 counts: What's next for the rap mogul?

Are you addicted to ‘fridge cigarettes’? Here’s what the Gen Z term means

RFK Jr. Brings MAHA to Oklahoma

St. Martin trio becomes the first females in Mississippi to sign Flag Football Scholarships

Federal investigation launched into Minnesota after transgender athlete leads team to championship

Democratic resolution to block military action in Iran fails to advance in US Senate

U.S. Senate prepares for passage of One Big Beautiful Bill Act | National

‘Hallowed ground, desecrated’: ICE sweeps at Chesterfield court draw fierce backlash

US Supreme Court allows SC to remove Planned Parenthood from list of Medicaid providers

Proposal to solve Tren de Aragua infiltration clears committee | North Carolina

Interview: Tupelo Police hosting summer D.A.R.E. camp
Building housing fireworks goes up in flames after electric box fire
Fireworks Safety Tips
Sean 'Diddy' Combs found guilty on 2 of 5 counts: What's next for the rap mogul?

Winter the Dolphin celebrated with new exhibit at Clearwater Marine Aquarium

Is ‘Jurassic World Rebirth’ worth the watch? Kathy Kaiser reviews!

CBS News Miami Special Report: FHP investigation shuts down I-95 during heavy rain

Fourth of July Firework Safety with AMR

Arkansas healthcare at risk in budget bill

Wednesday storms cause flooding, damage and crashes before moving out

What should Kentuckians expect ahead of a heavy travel weekend?
-

 News from the South - Georgia News Feed6 days ago
News from the South - Georgia News Feed6 days agoAre you addicted to ‘fridge cigarettes’? Here’s what the Gen Z term means
-
News from the South - Oklahoma News Feed7 days ago
RFK Jr. Brings MAHA to Oklahoma
-
Local News7 days ago
St. Martin trio becomes the first females in Mississippi to sign Flag Football Scholarships
-
News from the South - South Carolina News Feed6 days ago
Federal investigation launched into Minnesota after transgender athlete leads team to championship
-
 The Center Square5 days ago
The Center Square5 days agoU.S. Senate prepares for passage of One Big Beautiful Bill Act | National
-
News from the South - Tennessee News Feed5 days ago
Democratic resolution to block military action in Iran fails to advance in US Senate
-
News from the South - Virginia News Feed7 days ago
‘Hallowed ground, desecrated’: ICE sweeps at Chesterfield court draw fierce backlash
-
News from the South - Florida News Feed7 days ago
US Supreme Court allows SC to remove Planned Parenthood from list of Medicaid providers