theconversation.com – Keith Diaz, Associate Professor of Behavioral Medicine, Columbia University – 2025-05-21 08:02:00
A study published in *Circulation: Cardiovascular Quality and Outcomes* found that prolonged sedentary time after hospitalization for chest pain is linked to a higher risk of heart problems and death within a year. Patients who spent over 15 hours sedentary daily had more than double the risk compared to those who spent 12 hours sedentary. Replacing 30 minutes of sedentary time with moderate movement, such as walking, reduced this risk by 62%, while light movement cut it by 50%. Even replacing sedentary time with sleep lowered the risk. The study highlights the importance of movement in recovery from heart issues.
For patients hospitalized with chest pain, the amount of time they spend sedentary afterward is linked to a greater risk for more heart problems and death within a year. That’s the key finding of a new peer-reviewed study my colleagues and I published in the journal Circulation: Cardiovascular Quality and Outcomes.
We asked 609 emergency room patients experiencing chest pain — average age of 62 — to wear a physical activity monitor for 30 days after leaving the hospital. The monitor measured movements, sitting time and sleep throughout the day. We then followed patients for one year to track whether they had additional heart problems or died.
We found that patients who averaged more than 15 hours of sedentary behavior daily — which does not include sleep — were more than twice as likely to experience more heart problems or die in the year after discharge than patients who accrued a daily average of 12 hours of sedentary time.
But our goal wasn’t just to document that sitting is harmful. It was also to figure out what patients should do instead to lower their risk.
We found that replacing 30 minutes of sedentary time with moderate or vigorous movement, like brisk walking or running, was most beneficial. It was associated with a 62% lower risk of experiencing more heart problems or dying in the year after discharge. But we also found that replacing 30 minutes of sedentary time with just light movement, such as slow walking or housework, lowered the risk of heart problems and death by 50%.
Sleep was also a healthier option. Replacing 30 minutes of sedentary time with sleep lowered the risk of heart problems and death by 14%.
Clogged arteries could lead to a heart attack. Veronica Zakharova/Science Photo Library via Getty Images
Why it matters
Over 8 million people in the U.S. are admitted to the hospital with chest pain suggestive of acute coronary syndrome. annually. This covers a range of conditions involving reduced blood flow to the heart, including angina and heart attack.
Patients with acute coronary syndrome remain at high risk of having another heart problem even with optimal medical treatment.
The risk also remains high for patients with chest pain who are discharged without a diagnosis of acute coronary syndrome, as their unexplained chest pain may be a precursor to more serious heart problems. Given this risk, there is a need to identify risk factors that can be modified to improve a patient’s prognosis after hospitalization for chest pain.
In previous research, we found that patients with acute coronary syndrome had a fear of exercise and were sedentary, spending over 13 hours a day sitting.
Given that sedentary behavior has been linked to poor heart health in the general population, we were concerned that patients were unknowingly increasing their risk of having another heart problem.
Our latest findings confirm that sedentary time is a harmful behavior for these patients. But beyond telling patients to stop sitting so much, our work provides important guidance: Any movement, regardless of how intense, can be beneficial after hospitalization. This is especially relevant for people recovering from heart problems who may find exercise difficult or scary.
While exercise provides the best “bang for your buck” in terms of health benefits, our findings are good news for patients who may not have the time, ability or desire to exercise. And for those unable to fit in more movement, just getting an extra half hour of sleep is a small, doable step that can make a meaningful difference for your health after hospitalization.
What still isn’t known
Researchers don’t fully understand why sedentary time is harmful. Muscles help regulate blood sugar and lipid levels. It is thought that when muscles aren’t used, such as when patients sit for hours, this can lead to harmful elevations in blood sugar and lipids.
In turn, this can cause inflammation, plaque buildup in the arteries and organ damage. More research is needed to understand the biological mechanisms so that we can determine just how much movement is needed in a day.
What’s next
While our study highlights the potential risks of sedentary behavior after being hospitalized for chest pain, it was an observational study. Clinical trials are needed to confirm that replacing sedentary time with activity or sleep can improve prognosis.
The Research Brief is a short take on interesting academic work.
Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Centrist
This content is focused on a scientific study regarding health outcomes related to sedentary behavior in patients with chest pain and does not express political opinions or ideological stances. The article emphasizes evidence-based medical findings and practical health advice that are universally relevant, thereby maintaining a neutral tone without leaning left or right politically.
theconversation.com – Megan Donelson, Lecturer in Health Rhetorics, University of Dayton – 2025-08-25 07:08:00
The Make America Healthy Again (MAHA) movement, led by Robert F. Kennedy Jr., emphasizes personal responsibility for health, framing chronic illnesses, including autism, as largely preventable through lifestyle changes. MAHA’s rhetoric neglects systemic factors like genetics, environmental exposures, and inequalities in healthcare access, fueling concerns in disability and chronic illness communities about blame shifting from government to individuals. Critics highlight MAHA’s reduction in autism research funding and worry its approach could jeopardize essential support systems. The movement also employs tactics like questioning established science, undermining public trust in medicine. Though its goals of healthier environments are popular, MAHA’s underlying agenda raises ethical and social concerns.
Blaming poor health outcomes on lifestyle choices can obscure public health issues. Anadolu via Getty Images
The Make America Healthy Again movement has generated a lot of discussion about public health. But the language MAHA proponents use to describe health and disease has also raised concerns among the disability and chronic illness communities.
I’m a researcher studying the rhetoric of health and medicine – and, specifically, the rhetoric of risk. This means I analyze the language used by public officials, institutions, health care providers and other groups in discussing health risks to decode the underlying beliefs and assumptions that can affect both policy and public sentiment about health issues.
As a scholar of rhetoric and the mother of an autistic child, in the language of MAHA I hear a disregard for the humanity of people with disabilities and a shift from supporting them to blaming them for their needs.
Such language goes all the way up to the MAHA movement’s highest-level leader, Health and Human Services Secretary Robert F. Kennedy Jr. It is clearly evident in the report on children’s health published in May 2025 by the MAHA Commission, which was established by President Donald Trump and is led by Kennedy, as well as in the MAHA Commission’s follow-up draft recommendations, leaked on Aug. 15, 2025.
One key concept for understanding the MAHA movement’s rhetoric, introduced by a prominent sociologist named Ulrich Beck, is what sociologists now call individualization of risk. Beck argued that modern societies and governments frame almost all health risks as being about personal choice and responsibility. That approach obscures how policies made by large institutions – such as governments, for example – constrain the choices that people are able to make.
In other words, governments and other institutions tend to focus on the choices that individuals make to intentionally deflect from their own responsibility for the other risk factors. The consequence, in many cases, is that the institution is off the hook for any responsibility for negative outcomes.
Beck, writing in 1986, pointed to nuclear plants in the Soviet Union as an example. People who lived near them reported health issues that they suspected were caused by radiation. But the government denied the existence of any evidence linking their woes to radiation exposure, implying that lifestyle choices were to blame. Some scholars have identified a similar dynamic in the U.S. today, where the government emphasizes personal responsibility while downplaying the effects of public policy on health outcomes.
A shift in responsibility
Such a shift in responsibility is evident in how MAHA proponents, including Kennedy, discuss chronic illness and disabilities – in particular, autism.
In its May 2025 report on children’s health, the MAHA Commission describes the administration’s views on chronic diseases in children. The report notes that the increased prevalence in “obesity, diabetes, neurodevelopmental disorders, cancer, mental health, autoimmune disorders and allergies” are “preventable trends.” It also frames the “major drivers” of these trends as “the food children are eating, the chemicals they are exposed to, the medications they are taking, and various changes to their lifestyle and behavior, particularly those related to physical activity, sleep and the use of technology.”
Extensive research shows that genetics accounts for most of the risk of developing autism, but the MAHA Commission report discussed only lifestyle and environmental factors. Dusan Stankovic/E+ via Getty Images
There’s nothing inherently wrong with studying the environmental factors that might contribute to autism or other neurodevelopmental disorders. In fact, many researchers believe that autism is caused by complex interactions between genes and environmental factors. But here’s where Beck’s concept of individualization becomes revealing: While the government is clearly not responsible for the genetic causes of chronic diseases, this narrow focus on lifestyle and environmental factors implies that autism can be prevented if these factors are altered or eliminated.
While this may sound like great news, there are a couple of problems. First, it’s simply not true. Second, the Trump administration and Kennedy have canceled tens of millions of dollars in research funding for autism – including on environmental causes – replacing it with an initiative with an unclear review process. This is an unusual move if the goal is to identify and mitigate environmental risk factors And finally, the government could use this claim to justify removing federally funded support systems that are essential for the well-being of autistic people and their families – and instead focus all its efforts on eliminating processed foods, toxins and vaccines.
Even more worrisome is the implication that autism is a kind of damage caused by the environment rather than one of many normal variations in human neurological diversity – framing people with autism as a problem that society must solve.
How language encodes value judgments
Such logic sets off alarm bells for anyone familiar with the history of eugenics, a movement that began with the idea of improving America by making its people healthier and quickly evolved to make judgments about who is and is not fit to participate in society.
Kennedy’s explanation for the rise in autism diagnoses contradicts decades of research by independent researchers as well as assessments by the CDC.
Even if organic foods and a toxin-free household were the answer to reducing the prevalence of autism, the leaked MAHA Commission strategy report steers clear of recommending government regulation in industries such as food and agriculture, which would be needed to make these options affordable and widely available.
Instead, MAHA’s supposed interventions would remain lifestyle choices – and expensive ones, at that – left for individual families to make for themselves.
Just asking questions
Kennedy and other MAHA proponents also employ another powerful rhetorical tactic: raising questions about topics that have already reached a scientific consensus. This tactic frames such questions as pursuits of truth, but their purpose is actually to create doubt. This tactic, too, is evident in the MAHA Commission’s reports.
MAHA rhetoric thus continues a troubling trend in the anti-vaccine movement of calling all of science and Western medicine into question in order to further a specific agenda, regardless of the risks to public health.
The MAHA Commission’s goals are almost universally appealing – healthier food, healthier kids and a healthier environment for all Americans. But analyzing what is implied, minimized or left out entirely can illuminate a much more complex political and social agenda.
Extensive research shows that genetics accounts for most of the risk of developing autism, but the MAHA Commission report discussed only lifestyle and environmental factors. Dusan Stankovic/E+ via Getty Images
There’s nothing inherently wrong with studying the environmental factors that might contribute to autism or other neurodevelopmental disorders. In fact, many researchers believe that autism is caused by complex interactions between genes and environmental factors. But here’s where Beck’s concept of individualization becomes revealing: While the government is clearly not responsible for the genetic causes of chronic diseases, this narrow focus on lifestyle and environmental factors implies that autism can be prevented if these factors are altered or eliminated.
While this may sound like great news, there are a couple of problems. First, it’s simply not true. Second, the Trump administration and Kennedy have canceled tens of millions of dollars in research funding for autism – including on environmental causes – replacing it with an initiative with an unclear review process. This is an unusual move if the goal is to identify and mitigate environmental risk factors And finally, the government could use this claim to justify removing federally funded support systems that are essential for the well-being of autistic people and their families – and instead focus all its efforts on eliminating processed foods, toxins and vaccines.
Even more worrisome is the implication that autism is a kind of damage caused by the environment rather than one of many normal variations in human neurological diversity – framing people with autism as a problem that society must solve.
How language encodes value judgments
Such logic sets off alarm bells for anyone familiar with the history of eugenics, a movement that began with the idea of improving America by making its people healthier and quickly evolved to make judgments about who is and is not fit to participate in society.
Kennedy’s explanation for the rise in autism diagnoses contradicts decades of research by independent researchers as well as assessments by the CDC.
Even if organic foods and a toxin-free household were the answer to reducing the prevalence of autism, the leaked MAHA Commission strategy report steers clear of recommending government regulation in industries such as food and agriculture, which would be needed to make these options affordable and widely available.
Instead, MAHA’s supposed interventions would remain lifestyle choices – and expensive ones, at that – left for individual families to make for themselves.
Just asking questions
Kennedy and other MAHA proponents also employ another powerful rhetorical tactic: raising questions about topics that have already reached a scientific consensus. This tactic frames such questions as pursuits of truth, but their purpose is actually to create doubt. This tactic, too, is evident in the MAHA Commission’s reports.
MAHA rhetoric thus continues a troubling trend in the anti-vaccine movement of calling all of science and Western medicine into question in order to further a specific agenda, regardless of the risks to public health.
The MAHA Commission’s goals are almost universally appealing – healthier food, healthier kids and a healthier environment for all Americans. But analyzing what is implied, minimized or left out entirely can illuminate a much more complex political and social agenda.
Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Center-Left
The content critically examines the Make America Healthy Again (MAHA) movement and its leadership, particularly focusing on Health and Human Services Secretary Robert F. Kennedy Jr. and the Trump administration’s policies. It highlights concerns about shifting responsibility for public health from government institutions to individuals, critiques the downplaying of systemic issues, and warns against rhetoric that could harm disabled communities. The analysis aligns with a center-left perspective by emphasizing social responsibility, government accountability, and skepticism toward right-leaning health policy approaches that prioritize personal responsibility over structural support.
theconversation.com – Luke Keller, Professor of Physics and Astronomy, Ithaca College – 2025-08-22 07:27:00
For decades, astronomers believed the first stars were massive, short-lived, and composed only of hydrogen and helium, ending in supernovae without forming planets. However, two 2025 studies challenge this view. One simulation shows turbulence in early gas clouds caused fragmentation, allowing lower-mass stars to form. Another experiment reveals helium hydride (HeH⁺), previously thought inert, catalyzed early molecular hydrogen (H₂) formation, enhancing cooling and enabling smaller clouds to collapse. These findings suggest the earliest stars included low-mass stars that may still exist today, potentially hosting the first planets. Observational confirmation remains challenging due to their faintness.
For decades, astronomers have wondered what the very first stars in the universe were like. These stars formed new chemical elements, which enriched the universe and allowed the next generations of stars to form the first planets.
The first stars were initially composed of pure hydrogen and helium, and they were massive – hundreds to thousands of times the mass of the Sun and millions of times more luminous. Their short lives ended in enormous explosions called supernovae, so they had neither the time nor raw materials to form planets, and they should no longer exist for astronomers to observe.
At least that’s what we thought.
Two studies published in the first half of 2025 suggest that collapsing gas clouds in the early universe may have formed lower-mass stars as well. One study uses a new astrophysical computer simulation that models turbulence within the cloud, causing fragmentation into smaller, star-forming clumps. The other study – an independent laboratory experiment – demonstrates how molecular hydrogen, a molecule essential for star formation, may have formed earlier and in larger abundances. The process involves a catalyst that may surprise chemistry teachers.
As an astronomer who studies star and planet formation and their dependence on chemical processes, I am excited at the possibility that chemistry in the first 50 million to 100 million years after the Big Bang may have been more active than we expected.
These findings suggest that the second generation of stars – the oldest stars we can currently observe and possibly the hosts of the first planets – may have formed earlier than astronomers thought.
Primordial star formation
Video illustration of the star and planet formation process. Credit: Space Telescope Science Institute.
Stars form when massive clouds of hydrogen many light years across collapse under their own gravity. The collapse continues until a luminous sphere surrounds a dense core that is hot enough to sustain nuclear fusion.
Nuclear fusion happens when two or more atoms gain enough energy to fuse together. This process creates a new element and releases an incredible amount of energy, which heats the stellar core. In the first stars, hydrogen atoms fused together to create helium.
The new star shines because its surface is hot, but the energy fueling that luminosity percolates up from its core. The luminosity of a star is its total energy output in the form of light. The star’s brightness is the small fraction of that luminosity that we directly observe.
This process where stars form heavier elements by nuclear fusion is called stellar nucleosynthesis. It continues in stars after they form as their physical properties slowly change. The more massive stars can produce heavier elements such as carbon, oxygen and nitrogen, all the way up to iron, in a sequence of fusion reactions that end in a supernova explosion.
Supernovae can create even heavier elements, completing the periodic table of elements. Lower-mass stars like the Sun, with their cooler cores, can sustain fusion only up to carbon. As they exhaust the hydrogen and helium in their cores, nuclear fusion stops and the stars slowly evaporate.
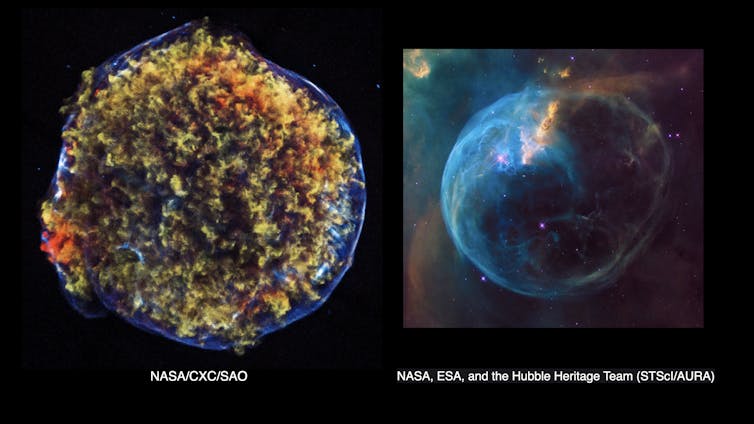
The remnant of a high-mass star supernova explosion imaged by the Chandra X-ray Observatory, left, and the remnant of a low-mass star evaporating in a blue bubble, right. CC BY
High-mass stars have high pressure and temperature in their cores, so they burn bright and use up their gaseous fuel quickly. They last only a few million years, whereas low-mass stars – those less than two times the Sun’s mass – evolve much more slowly, with lifetimes of billions or even trillions of years.
If the earliest stars were all high-mass stars, then they would have exploded long ago. But if low-mass stars also formed in the early universe, they may still exist for us to observe.
Chemistry that cools clouds
The first star-forming gas clouds, called protostellar clouds, were warm – roughly room temperature. Warm gas has internal pressure that pushes outward against the inward force of gravity trying to collapse the cloud. A hot air balloon stays inflated by the same principle. If the flame heating the air at the base of the balloon stops, the air inside cools and the balloon begins to collapse.
Only the most massive protostellar clouds with the most gravity could overcome the thermal pressure and eventually collapse. In this scenario, the first stars were all massive.
The only way to form the lower-mass stars we see today is for the protostellar clouds to cool. Gas in space cools by radiation, which transforms thermal energy into light that carries the energy out of the cloud. Hydrogen and helium atoms are not efficient radiators below several thousand degrees, but molecular hydrogen, H₂, is great at cooling gas at low temperatures.
When energized, H₂ emits infrared light, which cools the gas and lowers the internal pressure. That process would make gravitational collapse more likely in lower-mass clouds.
For decades, astronomers have reasoned that a low abundance of H₂ early on resulted in hotter clouds whose internal pressure would be too hot to easily collapse into stars. They concluded that only clouds with enormous masses, and therefore higher gravity, would collapse – leaving more massive stars.
Helium hydride
In a July 2025 journal article, physicist Florian Grussie and collaborators at the Max Planck Institute for Nuclear Physics demonstrated that the first molecule to form in the universe, helium hydride, HeH⁺, could have been more abundant in the early universe than previously thought. They used a computer model and conducted a laboratory experiment to verify this result.
Helium hydride? In high school science you probably learned that helium is a noble gas, meaning it does not react with other atoms to form molecules or chemical compounds. As it turns out, it does – but only under the extremely sparse and dark conditions of the early universe, before the first stars formed.
HeH⁺ reacts with hydrogen deuteride – HD, which is one normal hydrogen atom bonded to a heavier deuterium atom – to form H₂. In the process, HeH⁺ also acts as a coolant and releases heat in the form of light. So, the high abundance of both molecular coolants earlier on may have allowed smaller clouds to cool faster and collapse to form lower-mass stars.
Gas flow also affects stellar initial masses
In another study, published in July 2025, astrophysicist Ke-Jung Chen led a research group at the Academia Sinica Institute of Astronomy and Astrophysics using a detailed computer simulation that modeled how gas in the early universe may have flowed.
The team’s model demonstrated that turbulence, or irregular motion, in giant collapsing gas clouds can form lower-mass cloud fragments from which lower-mass stars condense.
The study concluded that turbulence may have allowed these early gas clouds to form stars either the same size or up to 40 times more massive than the Sun’s mass.
The galaxy NGC 1140 is small and contains large amounts of primordial gas with far fewer elements heavier than hydrogen and helium than are present in our Sun. This composition makes it similar to the intensely star-forming galaxies found in the early universe. These early universe galaxies were the building blocks for large galaxies such as the Milky Way. ESA/Hubble & NASA, CC BY-ND
The two new studies both predict that the first population of stars could have included low-mass stars. Now, it is up to us observational astronomers to find them.
This is no easy task. Low-mass stars have low luminosities, so they are extremely faint. Several observational studies have recently reported possible detections, but none are yet confirmed with high confidence. If they are out there, though, we will find them eventually.
The remnant of a high-mass star supernova explosion imaged by the Chandra X-ray Observatory, left, and the remnant of a low-mass star evaporating in a blue bubble, right. CC BY
High-mass stars have high pressure and temperature in their cores, so they burn bright and use up their gaseous fuel quickly. They last only a few million years, whereas low-mass stars – those less than two times the Sun’s mass – evolve much more slowly, with lifetimes of billions or even trillions of years.
If the earliest stars were all high-mass stars, then they would have exploded long ago. But if low-mass stars also formed in the early universe, they may still exist for us to observe.
Chemistry that cools clouds
The first star-forming gas clouds, called protostellar clouds, were warm – roughly room temperature. Warm gas has internal pressure that pushes outward against the inward force of gravity trying to collapse the cloud. A hot air balloon stays inflated by the same principle. If the flame heating the air at the base of the balloon stops, the air inside cools and the balloon begins to collapse.
Only the most massive protostellar clouds with the most gravity could overcome the thermal pressure and eventually collapse. In this scenario, the first stars were all massive.
The only way to form the lower-mass stars we see today is for the protostellar clouds to cool. Gas in space cools by radiation, which transforms thermal energy into light that carries the energy out of the cloud. Hydrogen and helium atoms are not efficient radiators below several thousand degrees, but molecular hydrogen, H₂, is great at cooling gas at low temperatures.
When energized, H₂ emits infrared light, which cools the gas and lowers the internal pressure. That process would make gravitational collapse more likely in lower-mass clouds.
For decades, astronomers have reasoned that a low abundance of H₂ early on resulted in hotter clouds whose internal pressure would be too hot to easily collapse into stars. They concluded that only clouds with enormous masses, and therefore higher gravity, would collapse – leaving more massive stars.
Helium hydride
In a July 2025 journal article, physicist Florian Grussie and collaborators at the Max Planck Institute for Nuclear Physics demonstrated that the first molecule to form in the universe, helium hydride, HeH⁺, could have been more abundant in the early universe than previously thought. They used a computer model and conducted a laboratory experiment to verify this result.
Helium hydride? In high school science you probably learned that helium is a noble gas, meaning it does not react with other atoms to form molecules or chemical compounds. As it turns out, it does – but only under the extremely sparse and dark conditions of the early universe, before the first stars formed.
HeH⁺ reacts with hydrogen deuteride – HD, which is one normal hydrogen atom bonded to a heavier deuterium atom – to form H₂. In the process, HeH⁺ also acts as a coolant and releases heat in the form of light. So, the high abundance of both molecular coolants earlier on may have allowed smaller clouds to cool faster and collapse to form lower-mass stars.
Gas flow also affects stellar initial masses
In another study, published in July 2025, astrophysicist Ke-Jung Chen led a research group at the Academia Sinica Institute of Astronomy and Astrophysics using a detailed computer simulation that modeled how gas in the early universe may have flowed.
The team’s model demonstrated that turbulence, or irregular motion, in giant collapsing gas clouds can form lower-mass cloud fragments from which lower-mass stars condense.
The study concluded that turbulence may have allowed these early gas clouds to form stars either the same size or up to 40 times more massive than the Sun’s mass.
The galaxy NGC 1140 is small and contains large amounts of primordial gas with far fewer elements heavier than hydrogen and helium than are present in our Sun. This composition makes it similar to the intensely star-forming galaxies found in the early universe. These early universe galaxies were the building blocks for large galaxies such as the Milky Way. ESA/Hubble & NASA, CC BY-ND
The two new studies both predict that the first population of stars could have included low-mass stars. Now, it is up to us observational astronomers to find them.
This is no easy task. Low-mass stars have low luminosities, so they are extremely faint. Several observational studies have recently reported possible detections, but none are yet confirmed with high confidence. If they are out there, though, we will find them eventually.
Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Centrist
This content is a scientific article focusing on astronomy and astrophysics, discussing recent research on the formation of the first stars in the universe. It presents factual information, references scientific studies, and avoids political or ideological language. The neutrality and objectivity in reporting scientific findings indicate no evident political bias, making it centrist in nature.
theconversation.com – David Higgins, Assistant Professor of Pediatrics, University of Colorado Anschutz Medical Campus – 2025-08-20 12:57:00
In August 2025, the American Academy of Pediatrics (AAP) issued new COVID-19 vaccine recommendations for children, diverging from the CDC’s guidance for the first time in 30 years. The AAP advises all children 6–23 months receive a full vaccine series and recommends a single dose for higher-risk children aged 2–18, while keeping vaccines available for others. This contrasts with the CDC’s “shared clinical decision-making” approach, which leaves vaccination decisions to families and providers. The divergence follows federal changes affecting vaccine advisory panels, raising concerns about CDC guidance credibility. Vaccine access, insurance coverage, and supply remain uncertain, potentially complicating implementation.
For 30 years, vaccine recommendations from the Centers for Disease Control and Prevention have aligned closely with those from the American Academy of Pediatrics, or AAP. But on Aug. 19, 2025, the AAP published new vaccine recommendations that diverge from those of the CDC.
The pediatrician association’s move comes on the heels of unprecedented changes made earlier this year by Robert F. Kennedy Jr., as head of the Department of Health and Human Services, in how the government approves and issues guidance on vaccines.
In a Q&A with The Conversation U.S., David Higgins, a pediatrician, preventive medicine physician and vaccine delivery researcher from the University of Colorado Anschutz Medical Campus, explains the new guidance and what it means for parents. Higgins is also a member of the American Academy of Pediatrics.
Pediatrician and preventive medicine specialist David Higgins explains the guidance in this video.
What are the AAP’s new vaccine recommendations?
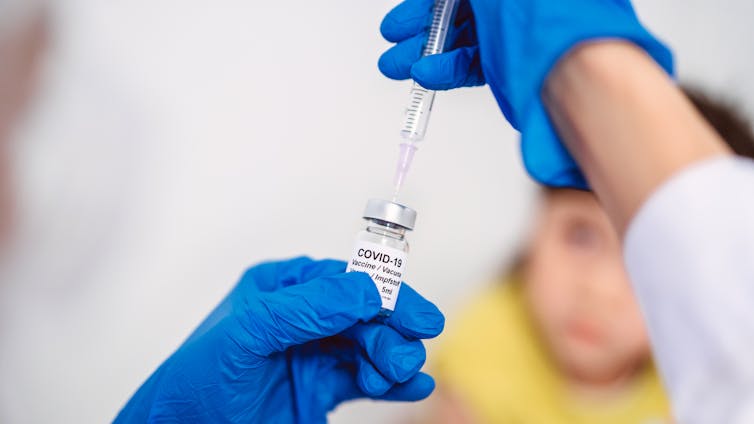
The AAP recommends that all children 6 to 23 months old receive a complete COVID-19 vaccine series, consistent with recommendations for this age group in previous years.
For children and adolescents ages 2 to 18, the AAP now advises a single dose if they are at higher risk, a change from previous years, when vaccination was recommended for all in this age group. Children at higher risk include those who have certain chronic medical conditions, who live in long-term care or group settings, who have never been vaccinated, or who live with family members at high risk.
The AAP also recommends that COVID-19 vaccines remain available for any child or adolescent whose parent wants them to be protected, regardless of risk status. In all cases, the most updated version of the vaccine should be used.
How do these recommendations differ from CDC guidance?
The difference is substantial. The CDC currently advises what it calls “shared clinical decision-making” for children ages 6 months to 17 years who are not moderately or severely immunocompromised. This means the decision is left up to individual discussions between families and their health care providers, but the vaccine is not treated as a routine recommendation. These current guidelines were made after Kennedy bypassed the agency’s normal independent review process.
That framework can be confusing for families and difficult for providers to implement. By contrast, the AAP recommendations identify the ages and conditions where the risk is highest while also supporting vaccine availability for any families who want it.
Will parents be able to follow these recommendations?
This is still unclear. The AAP recommendations do not automatically guarantee insurance coverage.
By law, insurance plans and the federal Vaccines for Children program, which provides vaccines for eligible children who might not otherwise be vaccinated due to cost or lack of insurance, are tied to Advisory Committee on Immunization Practices recommendations. Unless insurers and policymakers act to align with the AAP recommendations, there is a risk that parents would be forced to pay the costs out of pocket.
Vaccine supply may also be an issue. Currently, only two COVID-19 vaccines are available for children under 12. Moderna’s vaccine is approved only for children with at least one high-risk condition, while Pfizer’s authorization for younger children may not be renewed. If that happens, any remaining Pfizer doses for this age group may be unusable, leaving a shortfall in available vaccines for children.
Finally, implementation may differ depending on the type of provider. Some vaccine providers, such as pharmacists, operate under policies tied strictly to CDC recommendations, which may make it harder to follow AAP’s schedule unless rules are updated.
What happens next?
Parents and providers are likely to face continued confusion, just as COVID-19 cases rise as children return to school. Much will depend on whether the Advisory Committee on Immunization Practices updates its own recommendations at its upcoming meeting, expected in September, and whether pediatric COVID-19 vaccines remain available.
Until then, parents can speak with their pediatricians to understand the best protection for their children.
Will parents be able to follow these recommendations?
This is still unclear. The AAP recommendations do not automatically guarantee insurance coverage.
By law, insurance plans and the federal Vaccines for Children program, which provides vaccines for eligible children who might not otherwise be vaccinated due to cost or lack of insurance, are tied to Advisory Committee on Immunization Practices recommendations. Unless insurers and policymakers act to align with the AAP recommendations, there is a risk that parents would be forced to pay the costs out of pocket.
Vaccine supply may also be an issue. Currently, only two COVID-19 vaccines are available for children under 12. Moderna’s vaccine is approved only for children with at least one high-risk condition, while Pfizer’s authorization for younger children may not be renewed. If that happens, any remaining Pfizer doses for this age group may be unusable, leaving a shortfall in available vaccines for children.
Finally, implementation may differ depending on the type of provider. Some vaccine providers, such as pharmacists, operate under policies tied strictly to CDC recommendations, which may make it harder to follow AAP’s schedule unless rules are updated.
What happens next?
Parents and providers are likely to face continued confusion, just as COVID-19 cases rise as children return to school. Much will depend on whether the Advisory Committee on Immunization Practices updates its own recommendations at its upcoming meeting, expected in September, and whether pediatric COVID-19 vaccines remain available.
Until then, parents can speak with their pediatricians to understand the best protection for their children.
Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Center-Left
This content presents information about COVID-19 vaccine recommendations with a focus on public health and scientific expertise. It highlights concerns about governmental interference in health advisory processes and underscores the importance of independent scientific review, which aligns with a perspective that trusts established medical institutions and prioritizes evidence-based policy. The piece critiques changes made under a politically controversial figure while emphasizing the pediatric community’s stance without displaying partisan rhetoric, situating it slightly left of center due to the emphasis on expert-led health guidance and skepticism toward political disruption in health agencies.


















































{kind=link}