Mississippi Today
Q&A: Feminist author Caroline Criado-Perez talks about the sometimes-deadly lack of data on the female body

Note: This Q&A first published in Mississippi Today’s InformHer newsletter. Subscribe to our free women and girls newsletter to read stories like this monthly.
Caroline Criado-Perez, a feminist author and public speaker living in London, talked about her latest book, “Invisible Women,” last week at Lemuria Books in Jackson.
Her book, published in 2019, explores the gender data gap. From frustrating examples of a freezing office or a shelf out of reach, to deadly examples of an undiagnosed heart attack or crashing a car whose safety features don’t account for women’s measurements, Criado-Perez’s book is full of the real-world consequences of a world built without women in mind.
While the lack of research on the female body is an age-old problem, she argues, it becomes all the more pressing with the emergence of artificial intelligence and the increasing reliance on “Big Data.”
Criado-Perez is working on a new book about the reproductive journey of women, and how little science knows about it. She says she plans to use Mississippi as a case study. She sat down for an interview with Mississippi Today.
Editor’s note: This Q&A has been edited for length and clarity.
Mississippi Today: Tell us about the arc of your career and how you got to the point where you were writing your book “Invisible Women.”
Caroline Criado-Perez: Yeah so that’s a question with a very long answer. Really the story of me writing this book is the story of me becoming a feminist. I didn’t grow up as a feminist. I would say I was sort of anti-feminist – I was really quite misogynistic. And I think that was a very normal thing for young women in the ‘90s. I didn’t really identify with women and I just thought, you know, we’re all equal now and everyone should just stop complaining.
And it wasn’t until I went to university – I went as a mature student, I was 25 I think – and it was the first time I had to read any feminist analysis. And I had to read this book called Feminism and Linguistic Theory, which introduced me to the idea of the “generic masculine,” so, using “he” gender-neutrally or “man” gender-neutrally. The author of this book pointed to research that showed that when people hear these words or read these words, they think of men. And that completely blew my mind because it made me realize that I was picturing a man and I was incredibly shocked that I never noticed that, as a woman, that I’m just picturing men all the time.
That really kick-started the whole process for me because having had that realization, I started noticing it in other areas, where we act like we’re speaking gender-neutrally and we’re actually talking about men. So, after my first degree I went and studied feminist and behavioral economics and that is where I sort of discovered the whole economy is built around this mythical man – even though we speak about it being objective like a science. And there were various other bits and pieces I was doing that made me notice it in other areas and then finally I came across it in health, and that was when I was writing my first book. And that was when I started reading some research, the very early stages of my understanding of how much health and our knowledge of the human body is actually knowledge of the male body. That we’re not as good at diagnosing heart attacks in women as in men, and women are 50% more likely to be misdiagnosed if they have a heart attack. And more than anything I just couldn’t believe that this wasn’t on the front page of every newspaper, why did people not know this, why was everyone not talking about this – women are more likely to die if you have a heart attack: what?! And this is because we haven’t researched female bodies?
So that is how it ended up being a book. Essentially because I had all these things going around in my head and I felt like I was going crazy, that everyone was just blithely acting like we were speaking gender-neutrally when I knew we were talking about men. And just the fact that it was a huge, systematic issue, I knew that it wasn’t going to be an article – it had to be a book. Because it was just in everything.
MT: I’m interested in this term you use near the beginning of your book, “absent presence.” What is the experience of being defined by an absence, a negative space, a silence?
CP: I mean, I suppose for someone who recognizes the negative space, it’s intensely frustrating to know that there are all these gaps and all these silences that, as a society, we just skip over and we don’t notice that they’re there.
This is why I start the book with the Simone de Beauvoir quotation about representation being the work of men, and how they describe the world from their own point of view – which they confuse with the absolute truth. I f—–g love that quote so much. Because I feel like it sums up my book in a quotation because it’s not about these men having deliberately described the world and excluded women from it. They think that’s really what it is like. They think they’re really talking about the real world and they don’t see these absent presences, this silent figure of the woman.
But as a woman, you’re constantly knocking up against it, against the ways in which the world has not been designed for you. And having done the research I’ve done, I now experience the world in quite a different way than I did before, and it’s not a more comfortable way – it’s a much more uncomfortable way, because I’m constantly frustrated.
And of course, when it comes to health care it’s something that one thinks about a lot – you know, has this drug been tested in my body, is this the correct dosage for me, do they know how this drug interacts, and what if I’m on contraception, have they actually done any research? And nine times out of 10, no, they haven’t. Or they don’t know how the menstrual cycle might interact with it.
So it’s intensely frustrating and sometimes frightening, I think, to then just experience the world in which, for the most part, we are still speaking gender-neutrally when we’re talking about men.
MT: You talk about how this is an age-old problem – we live in a world made by men with men in mind. Can you tell us why, in a world that increasingly relies on “Big Data,” it matters so much more? How it becomes deadly, even?
CP: Yeah, so I mean, the gap in data for women is already deadly, if you’re thinking anywhere from car design to health care, but the real danger is becoming exponential, because of the introduction of AI into every single part of our world. And the problem with developing AI using bad data, biased data, is that machine learning is not like a human, in that it doesn’t simply reflect our biases back at us – it amplifies them.
I’ve read so many papers since “Invisible Women” came out where researchers will be like, “we’ve developed this AI and it performs better than a radiologist at detecting lung cancer” or “can predict heart attacks five years before they happen,” and then when you look at the paper, not only are the datasets incredibly male-biased, so you’ve got that bias already baked in, but also, they’re not even thinking about sex.
One paper I’m thinking about that came out shortly after “Invisible Women” was published was about predicting heart attacks. And there are sex-specific risk factors. So, if you’re going to be predicting heart attacks in men versus women, you don’t want to have, as this paper did, something like a 70% male dataset, but you even more don’t want to have that data all mixed up together. Because that’s not going to work for men or women. And yet, there was absolutely no mention of sex in the paper. So, that is frightening. Because the problem with that is it could make the situation worse.
When I find AI exciting is when researchers are using AI to address problems that we aren’t addressing otherwise. So, for example, one woman I spoke to was developing AI to detect victims of domestic violence via injury patterns, potentially years in advance of them ultimately having to be taken to a shelter or something. Because of course victims don’t necessarily report, and it’s not something that we’re investing a lot of money in in health care – because there’s not a lot of money in it and doctors don’t necessarily have the time to do the sort of questioning of a victim, et cetera. So there is exciting potential for AI. But if we’re just using it to do what we’re already doing but faster, that’s where the massive pitfalls are.
MT: As a health reporter, I’m interested in the subject of endocrine-disrupting chemicals you bring up in your book. We know that these chemicals are in everything, but they’re especially pervasive in feminine products, such as toiletries and makeup – and even menstrual products that women put inside their bodies. And as you know, not only are they more common in female products – they’re also worse for women, because of how they mimic and disrupt women’s hormones. How do we begin to address the issue? How can data help?
CP: The first thing that needs to change is obviously labeling – that’s a huge one, that people have the right to know what is actually in these products. That is one of the things that makes me most frustrated. I mean, as you can imagine, since writing the book I am scanning product ingredients all the time. If there’s anything that says “fragrance” I’m like “nope, that’s out, not using that.” And it’s amazing how many products just have these random ingredients in them and they don’t have to disclose what they are. Nobody knows. Nobody knows that “fragrance” means they could put anything in there. That’s deeply frustrating.
But my answer is always going to come back to: we have to collect data on this. And that is the thing that we’re not doing. And that is just incredible to me. The problem we have is not only are there endocrine-disrupting chemicals in these products, but also, how are these affecting not only the women who use them but also the women who work with them and the women who produce them.
And, as I say in my work, it’s not just that we haven’t tested them on women – for example, absorption into female skin, which can be different, or the way that it might accumulate in a female body, because of differences in fat in the body – but also the way in which women encounter them. Because it tends not to be in discrete “now I’m going to be exposed to this chemical, and tomorrow to that chemical.” We’re exposed to a cocktail of chemicals, and that’s not how they’re tested. So the way they’re tested is in itself biased against the way women are exposed to them, as well as the fact that we aren’t even testing them on women anyways.
And I feel that this really ties into this attitude that somehow the female workplace is this cozy, safe place, that women are never exposed to any form of danger. Because historically, the sort of headline-grabbing dangerous jobs have been done by men. By the way, because they were high-paying and women were barred from doing them, but let’s not let that get that in the way of the story that “women are lazy and they don’t want to do scary, difficult jobs.” But the female-dominated jobs that are low-paid, we simply have not been measuring how dangerous they are – from the perspective of exposure to chemicals.
MT: So, it seems like the call to action of this book is to begin filling in some of these gaps in data. But if we think of the modern world as being made up of data, then the idea of collecting all this new data can feel almost like building a new world – and that might be intimidating to some. What would you say to people who feel overwhelmed by this imperative?
CP: Well, there’s no getting around the fact that it is a huge job, and it is intimidating. And if you tried to do it all, you would be overwhelmed. But nobody could possibly fix this on their own. It’s like saying “you – go fix patriarchy.” It’s not how it works. Everybody has their own area that they can address. And so, people who work in research can collect sex disaggregated data. That’s a really great thing that people who work in research can do. People who work in HR, there’s a lot that they can do when it comes to looking at how their companies consider diversity, for example, in decision making.
People who have children, there’s so much that they can do to address how the future generation even notices that the “default male” operates. Like, if you look at kids’ TV, kids’ books, it’s “default male” all over the place – all the characters are male and if there’s a female character, her characteristic is that she’s female. I’m not saying that you’re going to be able to protect kids from that, but have a conversation with them. And I wish that had happened to me when I was little, that someone had taken the time to point out “isn’t it weird that in the real world, there’s all these women, and in your stories, it’s all boys?” I think that that’s a really powerful thing and I actually think that that’s something that everyone can do is have these conversations and notice when the “default male” is in operation – because I think that that really is half the battle.
If you think about the car crash stuff, that we have historically used an average male car crash test dummy, as if that’s representative of humans overall – when you say it like that, it obviously sounds ridiculous. But we’re so used to using the male body as the human body that people don’t even notice that it’s happening. As soon as you tell people “by the way, cars have not been tested to be safe for an average female body,” they understandably get really freaked out and start demanding change from car manufacturers – which is something very cool that’s happening in America at the moment. So, a really big part of it is just spreading the word and making the changes you can make.
MT: So, we’re talking about the gap in data around the female body and how that plays out in the health care system. One of the things I’ve noticed is that when people bring up this gap and try to address it – and particularly when talking about the menstrual cycle and how it interacts with medicine or what have you – that people tend to think of it as “woo-woo” or “mystical.” I think the fact that talking about something as fundamental as the menstrual cycle is met with such disbelief sheds light on just how uncommon it is to talk about the female body. Has that been your experience? Why is that?
CP: Right. That’s just sexism. It’s like, “oh, that has to do with ladies.” So, you’re reminding me of this report that came out, and again it was after “Invisible Women” was published, and it was about women and asthma. And there were all these testimonials from women who said “I went to the doctor and told them I feel like I get asthma flare-ups in relation to my menstrual cycle, I can tell where in my menstrual cycle I am, based on my flare-ups.” And the doctors were like “that’s just nonsense, you’re making it up” – because women can’t possibly know what’s going on with our bodies. Anyways, it transpires that actually, yes it is. It is hormonally-linked.
So that is something that, hashtag-not-all-doctors, but that they will say because there is this idea that lingers on somehow, in these people who are trained in science, that women are somehow just hysterical and should be less believed than men. But, I mean, that’s just misogyny.
MT: So you’re writing a new book. Tell us about how it relates to health care and how you’re using Mississippi as a case study.
CP: Yeah, so the book is about a woman’s reproductive journey from the beginning of whether or not she’s going to have children and going through things like pregnancy and how little we know about, firstly, how to treat a pregnant woman for anything, because we don’t do any research on women, let alone pregnant women. And then, how little we know about reproduction, so things like miscarriage and the disorders of pregnancy we know very little about, and of course that ties into abortion.
So that’s the area I’m wanting to focus on while I’m in Mississippi – for the obvious reason of Dobbs, and also my husband is from Mississippi, and also I had a miscarriage in January last year when we were last here, which was briefly scary, particularly as a British person, being here and thinking “if this goes wrong, am I going to be able to get the care I need?”
So I’m just really interested in understanding what it is actually like for a woman whose pregnancy goes wrong in Mississippi right now. Because I know there are these exceptions, but also, they’re never used. So, the focus for that chapter is I want to look at what happens to women who need an abortion and legally, supposedly, can get one, but actually, can’t get one. And then the rest of the book is looking at fertility and infertility through to the menopause.
This article first appeared on Mississippi Today and is republished here under a Creative Commons license.![]()











Tangled finances, thousands in personal loans and a political contribution from a supposed investor group made up of undercover FBI informants — this was all contained in a months-late campaign finance report from Hinds County District Attorney Jody Owens.
Owens, a second-term Democrat in Mississippi’s capital city region, is fighting federal bribery charges, to which he’s pleaded not guilty. At the same time, his recent campaign finance disclosure reflects a pair of transactions that correspond with key details in the government’s allegation that Owens took money from undercover informants to pay off a local official’s debt.
Regarding payments from Facility Solutions Team — the company name used in the FBI sting — to former Jackson City Councilwoman Angelique Lee, Owens allegedly stated the need to “clean it out,” according to the indictment, which was unsealed in November.
“[L]ike we always do, we’ll put it in a campaign account, or directly wire it,” he said, the indictment claims. “[T]hat’s the only way I want the paper trail to look.”
Agents recorded hundreds of hours of conversations with Owens and other officials, and after his arraignment last year, Owens responded to the charges, saying, “The cherry-picked statements of drunken locker room banter is not a crime.”
Throughout 2024, a non-election year during which federal authorities allege Owens funneled thousands of dollars in bribes to Jackson’s city officials, Owens loaned his campaign more than $20,000, according to his campaign committee’s finance report. He’d won reelection in late 2023.
Owens and his attorneys did not respond to questions about his campaign finance report.
Owens’ report, filed May 30 – months late and riddled with errors – is the latest example of how Mississippi politicians can ignore the state’s campaign finance transparency laws while avoiding meaningful consequences. It’s a lax legal environment that has led to late and illegible reports, untraceable out-of-state money that defied contribution limits, and, according to federal authorities, public corruption with campaign finance accounts serving as piggy banks.
Enforcement duties are divided among many government bodies, including the Mississippi Ethics Commission. The commission’s executive director, Tom Hood, has long complained that the state’s campaign finance laws are confusing and ineffective.
“It’s just a mess,” Hood said.
Owens filed the annual report months past the Jan. 31 deadline, after reporting from The Marshall Project – Jackson revealed he had failed to do so. He paid a $500 fine in April.
He was also late filing in previous years, paying fines in some years and failing to pay the penalties in other years, according to records provided by the Ethics Commission.
The report, which Owens signed, is full of omissions or miscalculations, with no way to tell which is which. The cover sheet of the report provides the total amount of itemized contributions and disbursements for the year — $44,000 in and $36,500 out. But the body of the report lists the line-by-line itemizations for each, and when the Marshall Project – Jackson and Mississippi Today summed the individual itemizations, the totals didn’t match those on the cover sheet.
Based on the itemized spending detailed in the body of the report, Owens’ campaign should have thousands more in cash on hand than reported. In the report’s cover sheet, Owens also reported that he received more in itemized contributions during the year than he received in total contributions, which would be impossible to do.
While the secretary of state receives and maintains campaign finance reports, it has no obligation to review the reports and no authority to investigate their accuracy. Under state law, willfully filing a false campaign finance report is a misdemeanor. Charges, however, are rare.
Owens is the only local official in the federal bribery probe — which is set to go to trial next summer — who remains in office. The government alleged that Owens accepted $125,000 to split between him and two associates in late 2023 from a group of men he believed were vying for a development project in downtown Jackson. Owens accepted several thousand dollars more to funnel to public officials for their support of the project, the indictment alleges. The use of campaign accounts was an important feature of the alleged scheme, according to the indictment.
Owens divvied up $50,000 from Facility Solutions Team, or FST, into checks from various individuals or companies — allegedly meant to conceal the bribe — to former Jackson Mayor Chokwe Lumumba’s reelection campaign, the indictment charged.
Lumumba accepted the checks during a sunset cruise on a yacht in South Florida, the indictment alleged. His campaign finance report, filed earlier this year, reflected five $10,000 contributions near the date of the trip, with no mention of FST.
Lumumba, who lost reelection in April, has pleaded not guilty.
While the indictment accused Owens of saying that public officials use campaign accounts to finance their personal lives, state law prohibits the use of political contributions for personal use.
The indictment alleges Owens accepted $60,000 — some for the purpose of funneling to local politicians — from the men representing themselves as FST in the backroom of Owens’ cigar bar on Feb. 13, 2024. On his campaign finance report, he listed a $12,500 campaign contribution from FST two days later, the same day the indictment alleges he paid off $10,000 of former Councilwoman Lee’s campaign debt. Lee pleaded guilty to charges related to the alleged bribery scheme in 2024.
Also on Feb. 15, 2024, the campaign finance report Owens filed shows a $10,000 payment to 1Vision, a printing company that used to go by the name A2Z Printing, for the purpose of “debt retirement.” Lee had her city paycheck garnished starting in 2023 to pay off debts to A2Z Printing, according to media reports. No mention of Lee was made in the campaign finance report filed by Owens. The printing company did not respond to requests for comment.
Campaigns are allowed to contribute money to other campaigns or political action committees. If Owens’ committee used campaign funds to pay off debt owed by Lee’s campaign, the transaction should have been structured as a contribution to Lee’s campaign and reported as such by both campaigns, said Sam Begley, a Jackson-based attorney and election law expert who has advised candidates about their financial disclosures.
The alleged debt payoff on behalf of Lee is not the first time Owens has described transactions on his campaign finance filings in ways that may obscure how his campaign is spending money. Confusing or unclear descriptions of spending activity are common on campaign finance reports across the state.
Owens previously reported that in 2023, he paid $1,275 to a staff member in the district attorney’s office who also worked on his campaign. The payment was labeled a reimbursement, which Owens explained in a May email to The Marshall Project – Jackson was for expenditures this person made on behalf of the campaign, “such as meals for volunteers/workers, evening/weekend canvassers, and election day workers.”
State law requires campaigns to itemize all contributions and expenses over $200. Begley said he believes Owens’ committee should have itemized any payments over $200 made by anyone on behalf of the campaign.
Upfront payments, with the expectation of repayment by the campaign, might also be considered a loan, according to a spokesperson for the secretary of state. Campaigns are barred from spending money to repay undocumented loans.
The state Ethics Commission has addressed undocumented loan repayments in several opinions, outlining the required documentation to make repayments legal.
Since 2018, the Ethics Commission has had the power to issue advisory opinions upon request to help candidates and campaigns sort through laws that Hood, the commission’s executive director, said aren’t always clear.
The commission has issued just six opinions in seven years.
“I was surprised in the first few years that there weren’t more,” Hood said. “But now it seems to be clear that for whatever reason, most people don’t think they need advice.”
This article first appeared on Mississippi Today and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
The post Indicted Jackson prosecutor's latest campaign finance report rife with errors appeared first on mississippitoday.org

Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Center-Left
The article critically examines the conduct of Hinds County District Attorney Jody Owens, a Democrat, and highlights systemic weaknesses in Mississippi’s campaign finance laws. While the reporting is grounded in factual evidence, legal documents, and expert commentary, the tone leans toward exposing flaws in enforcement and transparency—issues typically emphasized by center-left or reform-oriented journalism. The article does not display partisan rhetoric or ideological framing beyond its focus on accountability and legal integrity. Its publication by Mississippi Today and The Marshall Project, both known for investigative work with slight progressive leanings, further supports a Center-Left classification.
The Mississippi State Department of Health issued an alert Wednesday that cases of pertussis, or whooping cough, are climbing in the state.
The year-to-date number of cases in Mississippi ballooned to 80 as of July 10. That compares to 49 cases in all of 2024.
No whooping cough deaths have been reported. Ten people have been hospitalized related to whooping cough, seven of whom were children under 2 years old.
Cases have largely been clustered in northeast Mississippi. The region accounts for 40% of cases statewide.
The nation has also seen rising rates of whooping cough, though cases have been climbing less steeply than in Mississippi. About 15,000 whooping cough cases have been reported nationwide this year, according to the Centers for Disease Control and Prevention.
The highly contagious respiratory illness is named for the “whooping” sound people make when gasping for air after a coughing fit. It may begin like a common cold but can last for weeks or months. Babies younger than 1 year are at greatest risk for getting whooping cough, and can have severe complications that often require hospitalization.
Whooping cough cases fell in Mississippi after the COVID-19 pandemic began, but have since rebounded. This is likely due to people now taking fewer mitigation measures, like masking and remote learning, State Epidemiologist Renia Dotson said at the state Board of Health meeting July 9.
The majority of cases – 76% – have occurred in children. Of the 73 cases reported in people who were old enough to be vaccinated, 28 were unvaccinated. Of those 28 people, 23 were children.
“Vaccines are the best defense against vaccine preventable diseases,” State Health Officer Dr. Dan Edney said after the State Board of Health meeting.
Mississippi has long had the highest child vaccination rates in the country. But the state’s kindergarten vaccination rates have dropped since a federal judge ruled in 2023 that parents can opt out of vaccinating their children for school on account of religious beliefs.
The pertussis vaccination is administered in a five-dose series for children under 7 and booster doses for older children and adults. The health department recommends that pregnant women, grandparents and family or friends that may come in close contact with an infant should get booster shots to ensure they do not pass the illness to children, particularly those too young to be vaccinated.
Immunity from pertussis vaccination wanes over time, and there is not a routine recommendation for boosters.
State health officials also encourage vaccination against other childhood illnesses, like measles. While Mississippi has not reported any measles cases, Texas has had recent outbreaks.
The Mississippi Health Department offers vaccinations to children and uninsured adults at county health departments.
Correction 7/16/25: This story has been updated to reflect that the age of the seven hospitalized children is under 2 years old.
This article first appeared on Mississippi Today and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.
The post Whooping cough cases increase in Mississippi appeared first on mississippitoday.org
Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Centrist
This article presents a straightforward, fact-based account of rising whooping cough cases in Mississippi without ideological framing. It cites official sources such as the Mississippi State Department of Health and the Centers for Disease Control and Prevention, offering context, statistics, and public health recommendations. While it mentions a 2023 federal court ruling that allowed religious exemptions to vaccinations—a potentially contentious topic—it does so factually without editorializing or assigning blame. The overall tone remains neutral and informative, aligning with public health reporting rather than political advocacy.
The driver’s license office in Jackson has moved downtown as the Mississippi Department of Public Safety prepares to shift its headquarters from the capital city to suburban Rankin County.
The department last month announced it was closing the license office that had operated for decades next to its headquarters just off Interstate 55 at Woodrow Wilson Avenue, near the VA Medical Center.
The new office is at 430 State St., near Jackson’s main post office and a few blocks from the Capitol.
“This location provides easier access for those who live and work in the area and ensures we can continue offering vital driver services in a more convenient and accessible space within the city of Jackson,” said Bailey Martin, spokesperson for the Department of Public Safety.
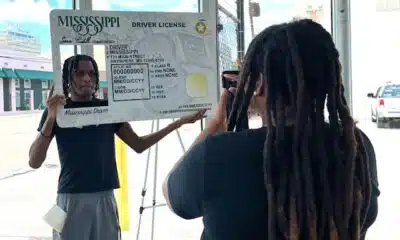
Mississippi has 35 driver’s licenses offices. The new Jackson office is in a former car dealership – an all-white building with floor-to-ceiling windows that fill the space with sunlight. On Wednesday, customers sat on black benches, chatting or scrolling on their phones while waiting to be called up to get or renew a license.
Carlos Lakes, 34, from Yazoo City, said he first went to the Richland office that issues commercial driver’s licenses but couldn’t get what he needed there. He said he then went to the old office on Woodrow Wilson and saw a note on the door showing the office had moved.
“So, it’s been about two hours of running around,” said Lakes, a truck driver.
He said the customer service at the new office was good, aside from the long wait time.
Medical student Seth Holton, 22, had a similar experience. He drove in from Flora, in Madison County, and went to the Woodrow Wilson location before finding the new office. He said it was his first time getting his license renewed.

“I think it looks nice,” Holton said of the new location. “I think it’s organized. There’s good seating. It’s pretty quick, for the most part.”
Student Marquerion Brown, 19, posed for photos with a large cardboard frame of a driver’s license in the corner of the new office. He’d just passed his driver’s test for the first time.
“I’m just lucky and thankful to get this one this time,” Brown said. He hadn’t decided where he wanted to drive first. “I got a lot of places in mind.”
The Department of Public Safety headquarters will open in Pearl within the next year, near the state’s crime lab, fire academy and emergency management agency.
Martin said the new headquarters will allow the department to have its divisions in one place – the highway patrol, bureau of investigation, bureau of narcotics, homeland security office and commercial transportation enforcement.
“As such, this move will enhance operational efficiency with other public safety partners, improve interagency collaboration, and position the department for future growth,” Martin said.
The headquarters move has been in the making for over five years. Public safety officials said the old building on Woodrow Wilson fell into disrepair after years of neglect.

Sen. David Blount, D-Jackson, was part of a group of lawmakers who proposed moving the headquarters to a different location inside Jackson.
“I personally think that the state government should be based in the state capital,” he said.
This article first appeared on Mississippi Today and is republished here under a Creative Commons Attribution-NoDerivatives 4.0 International License.![]()
The post Driver's license office moves to downtown Jackson appeared first on mississippitoday.org
Note: The following A.I. based commentary is not part of the original article, reproduced above, but is offered in the hopes that it will promote greater media literacy and critical thinking, by making any potential bias more visible to the reader –Staff Editor.
Political Bias Rating: Centrist
This article from *Mississippi Today* offers a factual and neutral report on the relocation of the Jackson driver’s license office and the broader headquarters move by the Mississippi Department of Public Safety. It includes quotes from officials and everyday citizens without editorializing or promoting a specific viewpoint. The inclusion of Sen. David Blount’s comment presents a mild political contrast, but it is balanced and not framed in a confrontational or ideological way. The tone remains focused on public service logistics and community impact rather than political narrative.

Judge limits a small part of a court order blocking Trump’s election overhaul as lawsuits continue

Intense storms downed power lines, left thousands in the dark across the Mid-South

Augusta Video Game Exposition set to return for 2026

What is Chronic Venous Insufficiency? Will Trump be okay?

Jackson County lawmakers override Frank White's vetoes

Indicted Jackson prosecutor’s latest campaign finance report rife with errors

Tomorrowland music festival opens after its main stage was destroyed by a huge fire

Ozarks weather whiplash in 2025 explained

Arrest made in school break-in, theft; another suspect still on the loose
WATCH LIVE | Friday Forecast

Bread sold at Walmart, Kroger stores in TN, KY recalled over undeclared tree nut

Man shot and killed in Benton County, near Rogers

Aiken County family fleeing to Mexico due to Trump immigration policies

Girls Hold Lemonade Stand for St. Jude Hospital | July 12, 2025 | News 19 at 10 p.m. – Weekend

Anti-ICE demonstrators march to Beaufort County Sheriff's Office

Police say couple had 50+ animals living in home

Coast judge upholds secrecy in politically charged case. Media appeals ruling.

Oyster spawning begins as MDMR-USM Hatchery Program enters production phase using mobile hatchery

Driver’s license office moves to downtown Jackson

Newswatch anchor Serena Davanzo says goodbye to the viewers
Intense storms downed power lines, left thousands in the dark across the Mid-South
What is Chronic Venous Insufficiency? Will Trump be okay?
Arrest made in school break-in, theft; another suspect still on the loose
WATCH LIVE | Friday Forecast

Alabama's Back-to-School Sales Tax Holiday returns: Which items are eligible

Christian's Morning Forecast: Strong Storms and Flood Watches Persist

Steps being taken to reopen parking garage at Harrison County Courthouse

Trump diagnosed with chronic ailment | FOX 5 News

Young photographer shoots for free, dedicated to his craft

Parking lot shoot out leaves 5 injured in Tower Grove South
-

 News from the South - Tennessee News Feed5 days ago
News from the South - Tennessee News Feed5 days agoBread sold at Walmart, Kroger stores in TN, KY recalled over undeclared tree nut
-
News from the South - Arkansas News Feed7 days ago
Man shot and killed in Benton County, near Rogers
-
News from the South - Georgia News Feed1 day ago
Aiken County family fleeing to Mexico due to Trump immigration policies
-
News from the South - Alabama News Feed6 days ago
Girls Hold Lemonade Stand for St. Jude Hospital | July 12, 2025 | News 19 at 10 p.m. – Weekend
-
News from the South - Georgia News Feed7 days ago
Anti-ICE demonstrators march to Beaufort County Sheriff's Office
-
News from the South - Oklahoma News Feed7 days ago
Police say couple had 50+ animals living in home
-
Mississippi Today4 days ago
Coast judge upholds secrecy in politically charged case. Media appeals ruling.
-
Local News5 days ago
Oyster spawning begins as MDMR-USM Hatchery Program enters production phase using mobile hatchery







