demaerre/iStock via Getty Images Plus
Kimberly Baker, Clemson University
With rising rates of obesity in the U.S. and increasing attention being paid to the health harms of processed foods, it’s clear that far more could be done to help consumers make healthy food choices.
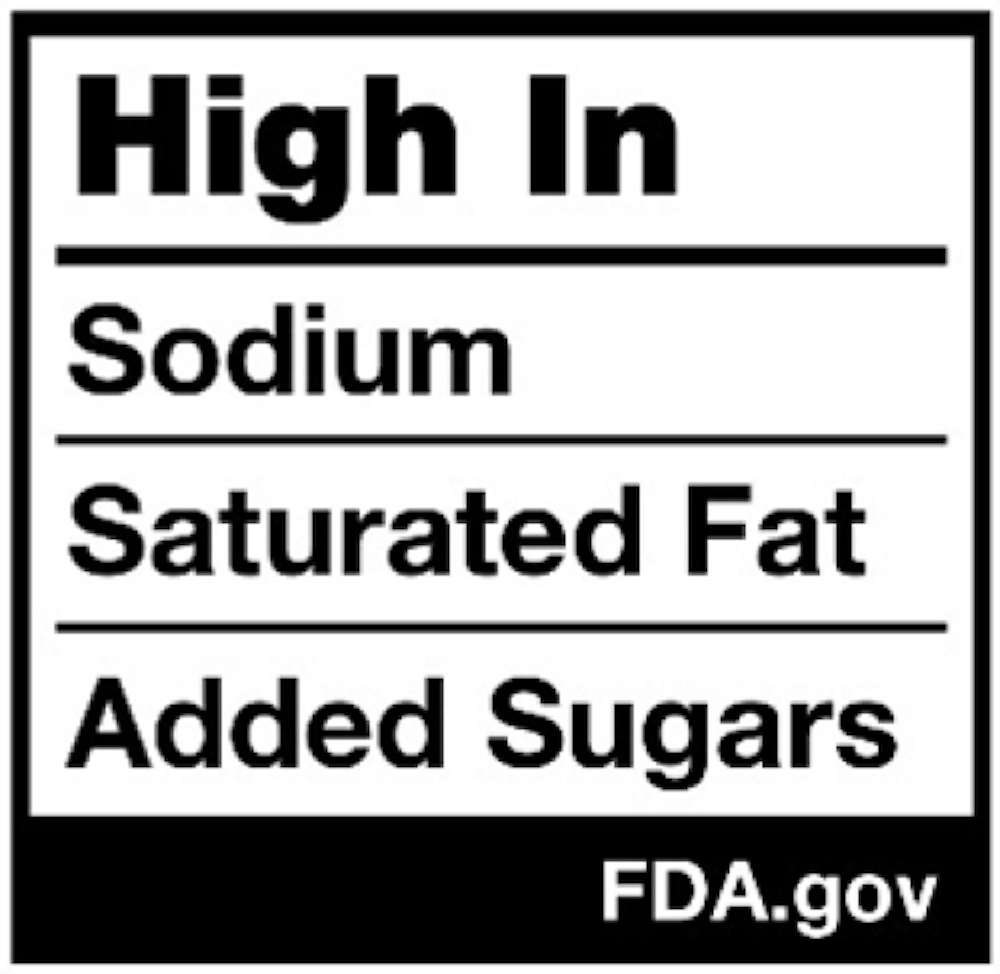
A bill known as the TRUTH in Labeling Act has been sitting before Congress since late 2023. If passed, it would require U.S. food manufacturers to add a second nutrition label to the front of product packages, in addition to the ones currently found on the back or side panel. It would also require the label to highlight any potentially unhealthy ingredients in the product, such as the amount of sugar, sodium and saturated fat it contains.
The proposed legislation would provide consumers with a standardized, easy-to-read and quick way to decide whether a product is a healthy choice. Should the bill, which is still in committee, become law, the front-of-package label would be regulated by the U.S. Food and Drug Administration.
The current nutrition facts label, typically featuring more detailed nutritional information and found on a product’s side panel, would remain unchanged.
As a food safety extension specialist who works with farmers, entrepreneurs, manufacturers and the government to help bring healthy food to shoppers, I believe that consistent front-of-package labeling would greatly benefit consumers by offering a straightforward way to compare multiple products, helping them make more informed choices.
Even if passed, it will take time for the FDA to interpret the law and standardize the design and format. And it might be years before all food manufacturers are required to use the new label. In the meantime, more than 175 million Americans are overweight or obese, and with each passing day, that number grows.
Why the change?
The newly proposed legislation is the latest effort by lawmakers to educate the public about smart food choices. Congress began requiring standardized nutrition labels on food packages through the Nutrition Labeling and Education Act of 1990.
FDA
But in the 34 years since that first label appeared, the obesity rate has more than tripled; 40% of Americans are now obese. Another 31% are overweight, and diet-related chronic illnesses, including heart disease, stroke, cancer, hypertension and Type 2 diabetes are rampant. About 60% of U.S. adults – 130 million people – have at least one of these chronic illnesses.
All of these diseases are associated with consuming too much sugar, sodium or saturated fat – three key ingredients the front label will focus on.
Labels help shoppers make better choices
There’s another reason to require a second, easy-to-notice, easy-to-comprehend label. Only about 40% of Americans frequently read the existing nutrition facts label; some shoppers say they don’t understand it. A simpler label with a more direct message might help those consumers. In fact, some studies suggest front-of-package labels do assist shoppers in making smart choices.
Research shows that those who frequently read the current label tend to have healthier diets than those who don’t. For example, frequent readers are almost four times more likely than rare readers to meet the recommended daily fiber intake.
Now the bad news: Even the frequent readers met their fiber goals only about 13% of the time. That isn’t good, but it’s an improvement over the rare readers, who meet their goals a paltry 3.7% of the time.
For the record, the daily recommendation for fiber is 25 grams for women and 38 for men under 50; its slightly less for those over 50.

FDA
Some foods still exempt
It’s possible you’ve already seen some front-of-package nutritional labels on food products. But these labels are not regulated by the government. Known as the “facts-up-front” labeling system, it’s strictly voluntary and a choice of the individual food manufacturer, with label designs and formats provided by the Consumer Brands Association, a trade association representing the food industry. Only a small number of manufacturers have chosen to put these labels on their products.
That said, more research is needed to know how long-term behavior may change due to front-of-package labeling. But at least one food safety advocacy organization, while supportive of front-of-package labels, says the trade association’s facts-up-front system is less than optimal.
Even if the TRUTH in Labeling Act passes as currently written, some foods could remain exempt from the nutritional label requirement, including fish, coffee, tea and spices.
There is one caveat, however. If any product makes a nutritional or health claim on its package – including those that are normally exempt – then a nutrition facts label must be on it.![]()
Kimberly Baker, Food Systems and Safety Program Team Director, Clemson University
This article is republished from The Conversation under a Creative Commons license. Read the original article.