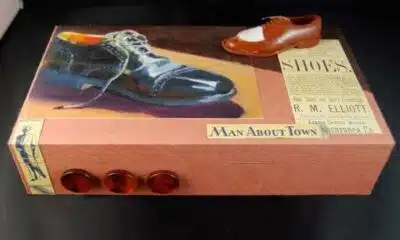
Spacewalks are among the more dangerous activities associated with human spaceflight.
Chris Impey, University of Arizona
Space is an unnatural environment for humans. We can’t survive unprotected in a pure vacuum for more than two minutes. Getting to space involves being strapped to a barely contained chemical explosion.
Since 1961, fewer than 700 people have been into space. Private space companies such as SpaceX and Blue Origin hope to boost that number to many thousands, and SpaceX is already taking bookings for flights to Earth orbit.
I’m an astronomer who has written extensively about space travel, including a book about our future off-Earth. I think a lot about the risks and rewards of exploring space.
As the commercial space industry takes off, there will be accidents and people will die. Polaris Dawn, planned to launch early in September 2024, will be a high-risk mission using only civilian astronauts. So, now is a good time to assess the risks and rewards of leaving the Earth.
Space travel is dangerous
Most Americans vividly recall the disasters that led to the loss of 14 astronauts’ lives. Two of the five space shuttles disintegrated, Challenger in 1986 soon after launch and Columbia in 2003 on reentry.
In total, 30 astronauts and cosmonauts have died while training for or during space missions.
There have also been dozens of close calls. Two astronauts are currently staying on the International Space Station for an extra six months because NASA declared their Boeing Starliner vehicle unsafe for the return journey. Starliner has had many problems during its development, including flammable tape, stuck valves and inadequate parachute systems. But a critical thruster malfunction is what caused NASA to abandon it as a return vehicle.
It’s not always safe on the ground, either. In addition to the three Apollo 1 astronauts who died in a 1967 launch pad fire, about 120 people died in the launchpad explosion of an unmanned rocket in Russia in 1960, and hundreds died in 1996 when a Chinese rocket veered off course and crashed into a nearby village.
The fatality rate of people traveling in space is about 3%. That sounds low, but it’s higher than extreme sports such as BASE jumping or jumping off a cliff wearing a wingsuit. The only recreations that rival the risk of space travel are solo free-climbing and climbing above 19,685 feet (6,000 meters) in the Himalayas.
Civilians in space
The 2020s have kicked off the era of civilian astronauts. After the death of schoolteacher Christa McAuliffe in the Challenger disaster, NASA stopped sending civilians into space. But for commercial space companies, it’s part of the business model.
The first all-civilian crew to reach orbit rode a SpaceX Dragon spacecraft in 2021, the Inspiration 4 mission. Since 2020, 69 private astronauts have gone to space, although only 46 reached the Kármán line – the formal definition of the edge of space.
The commercial space industry’s safety record is not perfect. No civilian has died in space, but one pilot died and another was seriously injured in a test flight of Virgin Galactic’s SpaceShipTwo craft in 2014. This accident followed three deaths and three injuries in an explosion during a prelaunch test of the SpaceShipTwo rocket in 2007.
SpaceX, the largest commercial space company with 13,000 employees and a market value of US$180 billion, has seen no fatalities in flight, but it has recorded one death and hundreds of injuries in the workplace.
The Polaris Dawn mission was planned to launch Aug. 27, 2024, though a helium leak and bad weather has delayed it. It will push the envelope of risk for civilians in space. This SpaceX flight will reach an altitude of 435 miles (700 kilometers), higher than any astronauts since Apollo.
The Polaris Dawn crew during their launch-day rehearsal.
The Polaris Dawn’s four-person civilian crew will receive a hefty dose of radiation, getting as much in a few hours as they would in 20 years on the Earth. NASA is doing research to understand the extent of the health risks from radiation.
The mission will also include a spacewalk – the first for nongovernment astronauts. It will use spacesuits never tested in space. Since the spacecraft they’re using – the SpaceX Dragon – has no airlock, the inside of the capsule will be exposed to the vacuum of space, with all the crew members wearing spacesuits.
Russian cosmonaut Alexei Leonov nearly died during the first spacewalk in 1965, and other spacewalks have led to temporary blindness, near drowning and nearly being lost in space forever. A spacesuit is like a miniature spacecraft, and it has to withstand rapid temperature changes of hundreds of degrees when moving in and out of direct sunlight. Even a small tear or puncture can be fatal.
But while space travel comes with dangers, it also has rewards. Since Polaris Dawn will travel higher than any previous mission that did not go to the Moon, the crew will be able to do research on high-radiation environments. They will investigate the effects of spaceflight on the human body and evaluate how future deep-space travelers might diagnose and treat themselves.
A less tangible but potentially profound benefit is the overview effect – many astronauts report a feeling of awe from experiencing the Earth from space.
Space boom
Space is booming – hopefully just metaphorically and not literally. SpaceX makes money by launching Starlink satellites and ferrying supplies and people to the International Space Station, with estimated revenues of $15 billion this year. Blue Origin sells rocket engines and has contracts with NASA.
Both companies sell rides into space to high-net-worth individuals, but that’s a small fraction of their revenues. Space tourism is not available to the masses yet. Virgin Galactic offers a short, suborbital ride for $450,000, but getting to Earth orbit will cost you $55 million.
The space tourism market was $750 million in 2023, and that’s projected to grow to $5.2 billion over the next decade. Reusable rockets have made the cost of launching a spacecraft 10 times cheaper than it was a decade ago.
For space tourism to take off with a demographic broader than multimillionaires and thrill-seekers, it needs to be safe – both in perception and in reality. Many space entrepreneurs expect space travel to follow aviation’s arc, which also started by attracting rich people and thrill-seekers.
Since 1930, improvements in technology and safety features have lowered the number of fatal accidents in the aviation industry per million miles flown by a factor of 3,000. A more realistic target may be to make space travel as safe as driving. That’s a more lenient target, since driving is more dangerous than flying. Your annual odds of dying in a car crash are 1 in 5,000, compared with annual odds of 1 in 11 million of dying in a plane crash.
In the United States, the government has kept regulations light on the commercial space industry to encourage entrepreneurs.
Elon Musk’s dreams of millions of passengers and a city on Mars may not become reality. But if the cost of a jaunt to Earth’s orbit comes down to the cost of a high-end cruise, many people could experience the thrill of weightlessness and of seeing the Earth as a beautiful planet from above.![]()
Chris Impey, University Distinguished Professor of Astronomy, University of Arizona
This article is republished from The Conversation under a Creative Commons license. Read the original article.