Richard Gunderman, Indiana University
With over 40 armed conflicts now taking place around the world, the costs of warfare are immense and continue to mount with each passing day.
Russia’s war on Ukraine is estimated to have resulted in more than 600,000 Russian casualties, with estimates of total dead and injured on both sides as high as 1 million. The war between Israel and Hamas has resulted in about 140,000 Palestinian and 10,000 Israeli casualties, and there have been at least 50,000 casualties in the ongoing Sudanese Civil War. Closer to home, the newly married son of a colleague of mine suffered grievous injuries and lost all four limbs in an explosion while serving in the Middle East.
The loss of life and limb, violations of human rights, destruction of personal property and damage to infrastructure such as power stations, hospitals and roads render such costs essentially incalculable, at least in monetary terms.
Yet war also opens up opportunities to care for the injured, displaced and forgotten. As someone who studies and writes about the intersection of medicine and the humanities, I often find myself returning to the American poet Walt Whitman.
To appreciate the act of offering support and comfort for the victims of war, there are few better sources of inspiration than Whitman, who spent more than three years volunteering his time and energies during the U.S. Civil War.
Compelled to help
Walt Whitman is considered one of the greatest poets in American history. Born the second of nine children in straitened circumstances in New York in 1819, he left school at age 11 to help support his family, working in a variety of jobs, including typesetting, teaching and newspaper publishing.
In 1855, he self-published his greatest work of poetry, “Leaves of Grass,” written in free verse and opening with the poem later known as “Song of Myself.” The work’s fans included Ralph Waldo Emerson, who wrote to Whitman, in a letter praising the poet, “I greet you at the beginning of a great career.”
A portrait of Walt Whitman from 1863, when the U.S. was embroiled in civil war.
Yet fame and fortune were slow to wend their way to Whitman, and he continued to work in the newspaper trade. With the onset of the Civil War, Whitman’s brother enlisted, and when Whitman saw his brother named among wounded soldiers, he traveled to Virginia to find him.
He eventually discovered that his brother had suffered only a minor wound. Yet during the search, Whitman encountered scores of wounded soldiers and piles of amputated limbs, which moved him to help in some way.
He secured a job in Washington, D.C., as an army paymaster’s clerk and began volunteering in the city’s military hospitals, making, by his estimate, over 600 visits, sometimes overnight, to as many as 100,000 soldiers.
Dispenser of treats, transcriber of letters
Why would perhaps America’s greatest poet voluntarily devote the better part of over three years of his life to visiting places replete with mutilation, agony and sorrow?
Lacking formal training in medicine or nursing, Whitman nonetheless felt that he had something important to offer.
“I found it was in the simple matter of personal presence, and emanating ordinary cheer and magnetism, that I succeeded and helped more than by medical nursing, or delicacies, or gifts of money, or anything else,” he wrote in “Memoranda During the War.”
Whitman managed to bring more tangible gifts as well: “Blackberries, peaches, lemons and sugar, wines, all kinds of preserves, pickles, brandy, milk, shirts and all articles of underclothing, tobacco, tea, and handkerchiefs.”
He procured these items using his own meager funds and by soliciting donations, providing others their own opportunities to give.
Consider a specific case, that of a young soldier from Massachusetts suffering from respiratory and gastrointestinal ailments.
Of him, Whitman wrote, “His heart was broken. He felt the struggle to keep up any longer to be useless. God, the world, humanity, all had abandoned him. It would feel so good to shut his eyes forever on the cruel things around him and toward him.”
Yet Whitman took his place beside him, gave him some money so that he could buy milk, and wrote a letter for him to his sister. “Trifling as it was, he was overcome and began to cry. He has told me since that this little visit, at that hour, just saved him – a day more, and it would have been perhaps too late.”
Along with all the other gifts in his haversack, Whitman “always gave paper, envelopes, and stamps” so soldiers could write to loved ones back home. Many times, he wrote their letters himself, in his own hand, often signing below their name, “Written by Walt Whitman, a friend.”
Of the letters, he noted:
“Many sick and wounded soldiers have not written home to parents, brothers, sisters, and even wives, for one reason or another, for a long time. Some are poor writers, some cannot get paper and envelopes; many have an aversion to writing because they dread to worry the folks at home – the facts about them are so sad to tell. I always encourage the men to write, and promptly write for them.”
It is remarkable to think of one of the greatest artists of the English language sitting by the bedside of so many sick and wounded soldiers, helping them compose letters to family and friends far away, sometimes simply transcribing what they said, and other times capturing what they wanted to say or what needed to be said.
He was tending not only to the soldiers before him, but also to loved ones sick with worry, hundreds of miles away.
Becoming conduits of compassion
Whitman’s dedicated service offers deep and enduring lessons for people around the world today.
The second page of a letter Walt Whitman wrote on behalf of Union soldier Robert N. Jabo, who was dying of tuberculosis. It was signed, ‘Written by Walt Whitman, a friend.’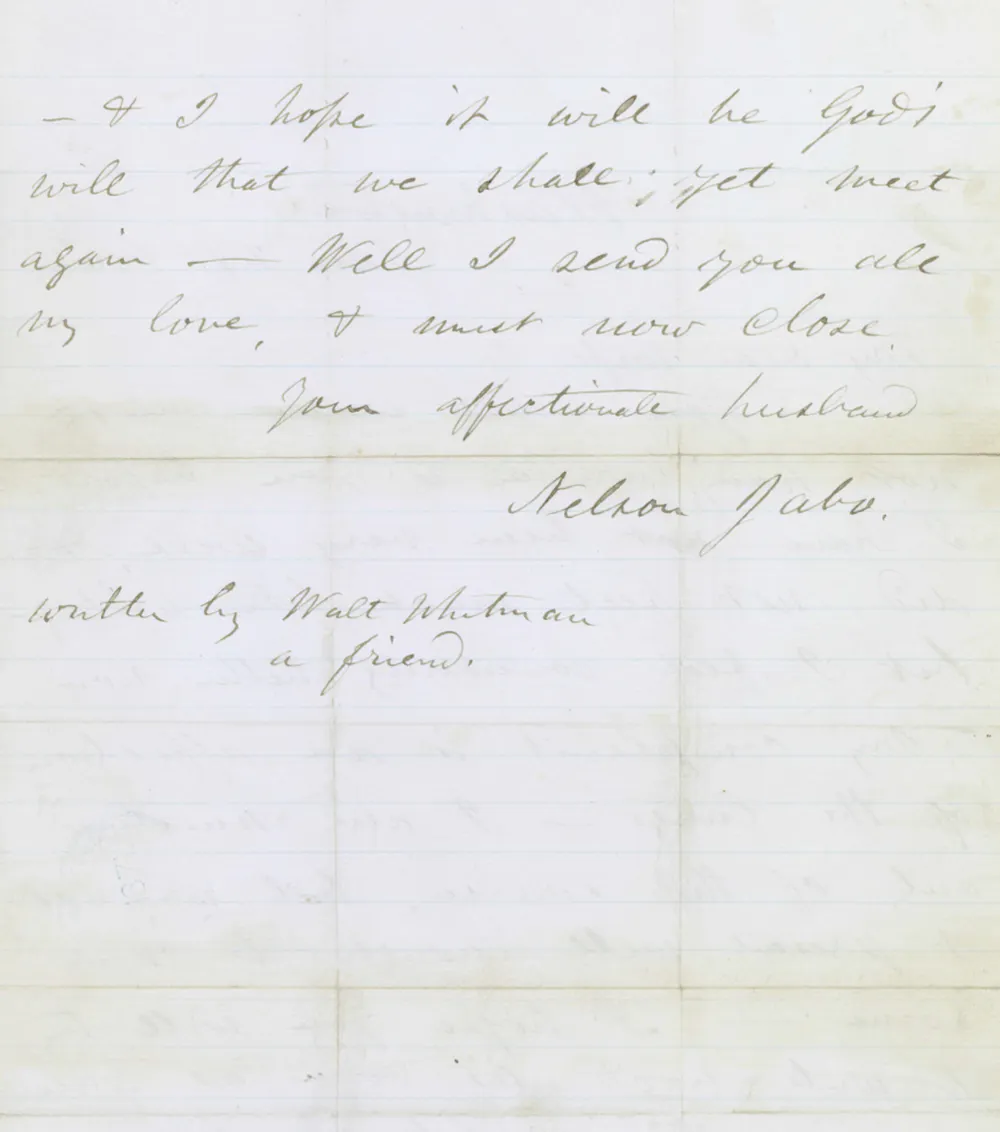
For one thing, the toll of war cannot simply be counted up in numbers of lives lost or billions of dollars of damage incurred.
Behind every number is a human story. Every wounded or dead soldier is someone’s son or daughter, sister or brother, husband or wife, or mother or father. Every civilian casualty is someone’s friend, neighbor and fellow citizen.
Whitman didn’t use his poetic powers just to help share the stories of wounded soldiers with their loved ones back home. He also mined his experiences by their bedside to compose literary masterpieces such as “The Wound-Dresser” and “Come Up from the Fields Father.”
As violence permeates the globe, it’s easy to look away, or become numb to headlines and images of death and despair. But confronting this suffering head on – through an act as simple as extending a hand, a voice or an ear – is an act of courage in and of itself.
True, it may not stop or win a war. Yet this sort of attention is a form of generosity and a conduit to healing – a way, as Whitman put it in a letter to his brother, “to have our feelings so thoroughly and permanently absorbed, to the very roots, by these huge swarms of dear, wounded, sick, and dying boys.”![]()
Richard Gunderman, Chancellor’s Professor of Medicine, Liberal Arts, and Philanthropy, Indiana University
This article is republished from The Conversation under a Creative Commons license. Read the original article.